

Financial toxicity of cancer treatment in India: towards closing the cancer care gap
- PMID: 37404274
- PMCID: PMC10316647
- DOI: 10.3389/fpubh.2023.1065737
Financial toxicity of cancer treatment in India: towards closing the cancer care gap
Abstract
Background: The rising economic burden of cancer on patients is an important determinant of access to treatment initiation and adherence in India. Several publicly financed health insurance (PFHI) schemes have been launched in India, with treatment for cancer as an explicit inclusion in the health benefit packages (HBPs). Although, financial toxicity is widely acknowledged to be a potential consequence of costly cancer treatment, little is known about its prevalence and determinants among the Indian population. There is a need to determine the optimal strategy for clinicians and cancer care centers to address the issue of high costs of care in order to minimize the financial toxicity, promote access to high value care and reduce health disparities.
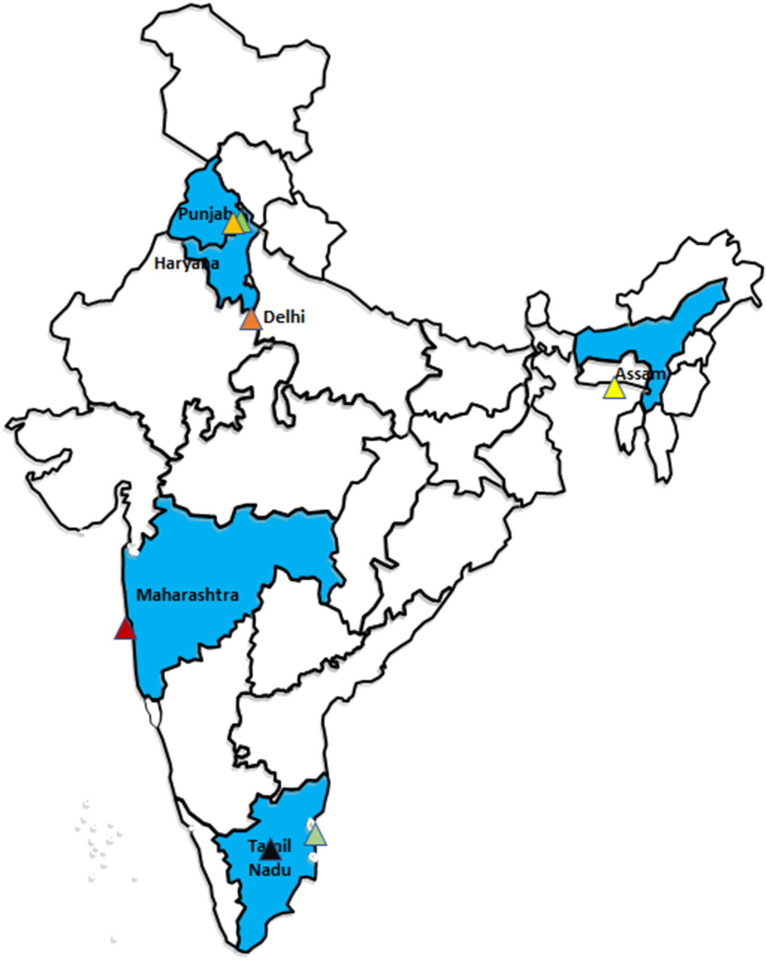
Methods: A total of 12,148 cancer patients were recruited at seven purposively selected cancer centres in India, to assess the out-of-pocket expenditure (OOPE) and financial toxicity among cancer patients. Mean OOPE incurred for outpatient treatment and hospitalization, was estimated by cancer site, stage, type of treatment and socio-demographic characteristics. Economic impact of cancer care on household financial risk protection was assessed using standard indicators of catastrophic health expenditures (CHE) and impoverishment, along with the determinants using logistic regression.
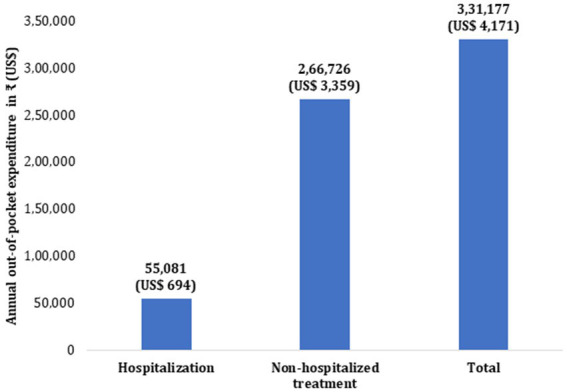
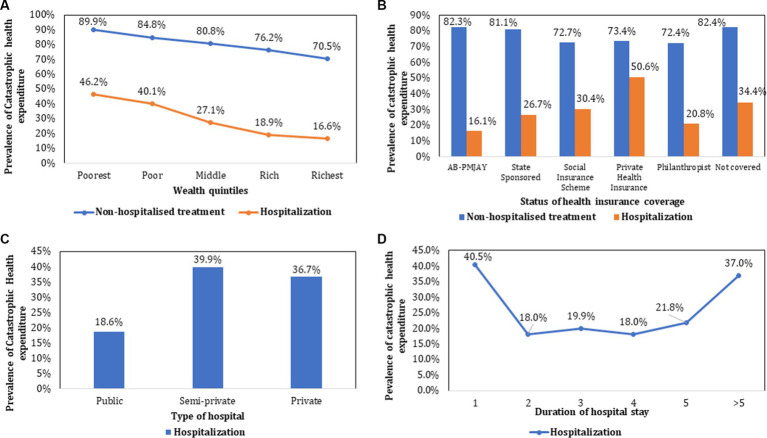
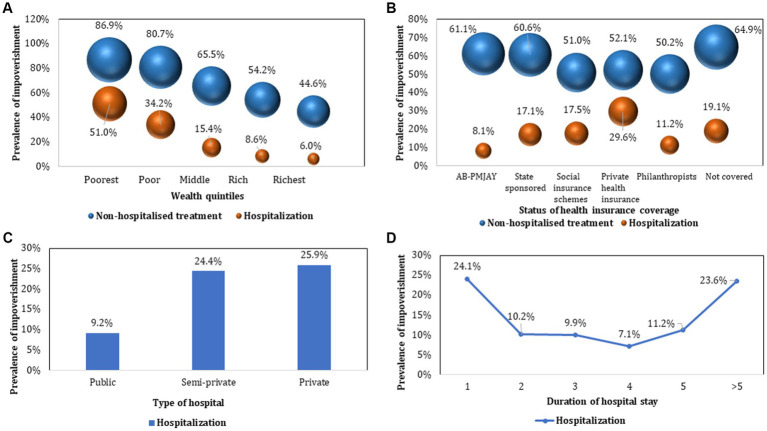
Results: Mean direct OOPE per outpatient consultation and per episode of hospitalization was estimated as ₹8,053 (US$ 101) and ₹39,085 (US$ 492) respectively. Per patient annual direct OOPE incurred on cancer treatment was estimated as ₹331,177 (US$ 4,171). Diagnostics (36.4%) and medicines (45%) are major contributors of OOPE for outpatient treatment and hospitalization, respectively. The overall prevalence of CHE and impoverishment was higher among patients seeking outpatient treatment (80.4% and 67%, respectively) than hospitalization (29.8% and 17.2%, respectively). The odds of incurring CHE was 7.4 times higher among poorer patients [Adjusted Odds Ratio (AOR): 7.414] than richest. Enrolment in PM-JAY (CHE AOR = 0.426, and impoverishment AOR = 0.395) or a state sponsored scheme (CHE AOR = 0.304 and impoverishment AOR = 0.371) resulted in a significant reduction in CHE and impoverishment for an episode of hospitalization. The prevalence of CHE and impoverishment was significantly higher with hospitalization in private hospitals and longer duration of hospital stay (p < 0.001). The extent of CHE and impoverishment due to direct costs incurred on outpatient treatment increased from 83% to 99.7% and, 63.9% to 97.1% after considering both direct and indirect costs borne by the patient and caregivers, respectively. In case of hospitalization, the extent of CHE increased from 23.6% (direct cost) to 59.4% (direct+ indirect costs) and impoverishment increased from 14.1% (direct cost) to 27% due to both direct and indirect cost of cancer treatment.
Conclusion: There is high economic burden on patients and their families due to cancer treatment. The increase in population and cancer services coverage of PFHI schemes, creating prepayment mechanisms like E-RUPI for outpatient diagnostic and staging services, and strengthening public hospitals can potentially reduce the financial burden among cancer patients in India. The disaggregated OOPE estimates could be useful input for future health technology analyses to determine cost-effective treatment strategies.
Keywords: cancer; catastrophic health expenditure; direct out of pocket expenditure; financial toxicity; hospitalization; impoverishment; indirect cost due to loss of productivity; outpatient care.
Copyright © 2023 Prinja, Dixit, Gupta, Dhankhar, Kataki, Roy, Mehra, Kumar, Singh, Malhotra, Goyal, Rajsekar, Krishnamurthy and Gupta.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Effectiveness of government strategies for financial protection against costs of hospitalization Care in India.BMC Public Health. 2018 Apr 16;18(1):501. doi: 10.1186/s12889-018-5431-8. BMC Public Health. 2018. PMID: 29661233 Free PMC article.
-
Role of publicly funded health insurance in financial protection of the elderly from hospitalisation expenditure in India-findings from the longitudinal aging study.BMC Geriatr. 2022 Jul 12;22(1):572. doi: 10.1186/s12877-022-03266-2. BMC Geriatr. 2022. PMID: 35820859 Free PMC article.
-
Is health insurance really benefitting Indian population? Evidence from a nationally representative sample survey.Int J Health Plann Manage. 2024 Mar;39(2):293-310. doi: 10.1002/hpm.3716. Epub 2023 Nov 1. Int J Health Plann Manage. 2024. PMID: 37910629
-
Cancer care and economic burden-A narrative review.J Family Med Prim Care. 2023 Dec;12(12):3042-3047. doi: 10.4103/jfmpc.jfmpc_1037_23. Epub 2023 Dec 21. J Family Med Prim Care. 2023. PMID: 38361876 Free PMC article. Review.
-
Economic Burden of Chronic Ill Health and Injuries for Households in Low- and Middle-Income Countries.In: Jamison DT, Gelband H, Horton S, Jha P, Laxminarayan R, Mock CN, Nugent R, editors. Disease Control Priorities: Improving Health and Reducing Poverty. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 27. Chapter 6. In: Jamison DT, Gelband H, Horton S, Jha P, Laxminarayan R, Mock CN, Nugent R, editors. Disease Control Priorities: Improving Health and Reducing Poverty. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 27. Chapter 6. PMID: 30212160 Free Books & Documents. Review.
Cited by
-
Spotlight on Lung Cancer Disparities in India.JCO Glob Oncol. 2025 Feb;11:e2400327. doi: 10.1200/GO-24-00327. Epub 2025 Feb 7. JCO Glob Oncol. 2025. PMID: 39919262 Free PMC article. No abstract available.
-
Economic Burden of Healthcare Services on Cancer Survivors in Bangladesh.Cancer Rep (Hoboken). 2024 Aug;7(8):e2144. doi: 10.1002/cnr2.2144. Cancer Rep (Hoboken). 2024. PMID: 39118451 Free PMC article.
-
Global, regional and country burden of high BMI-related liver cancer among individuals aged above 70: trends from 1990 to 2021 and projections to 2044.Front Public Health. 2025 Mar 20;13:1523578. doi: 10.3389/fpubh.2025.1523578. eCollection 2025. Front Public Health. 2025. PMID: 40182530 Free PMC article.
-
Healthcare utilisation and economic burden of cancer on Indian households.Sci Rep. 2025 May 14;15(1):16780. doi: 10.1038/s41598-025-01279-6. Sci Rep. 2025. PMID: 40368978 Free PMC article.
-
Exploring adaptive health technology assessment for evaluating 10 cancer interventions: insights and lessons from a pilot study in India.BMJ Evid Based Med. 2025 Jan 2:bmjebm-2023-112490. doi: 10.1136/bmjebm-2023-112490. Online ahead of print. BMJ Evid Based Med. 2025. PMID: 39746782
References
-
- WHO . Cancer Fact Sheet. WHO Newsroom. Available at: https://www.who.int/news-room/fact-sheets/detail/cancer (Accessed June 20, 2022).
-
- WHO . Cancer. WHO Health Topics. Available at: https://www.who.int/health-topics/cancer#tab=tab_1 (Accessed June 20, 2022).
-
- IARC . Q&A World Cancer Report. Available at: https://www.iarc.who.int/world-cancer-report-qa-weiderpass_wild/ (Accessed June 20, 2022).
-
- International Agency for Research on Cancer . World Health Organization. GLOBOCAN 2018 – India. Available at: https://gco.iarc.fr/today/data/factsheets/populations/356-india-fact-she... (Accessed July 21, 2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous