

Obinutuzumab Versus Rituximab Immunochemotherapy in Previously Untreated iNHL: Final Results From the GALLIUM Study
- PMID: 37404773
- PMCID: PMC10317485
- DOI: 10.1097/HS9.0000000000000919
Obinutuzumab Versus Rituximab Immunochemotherapy in Previously Untreated iNHL: Final Results From the GALLIUM Study
Abstract
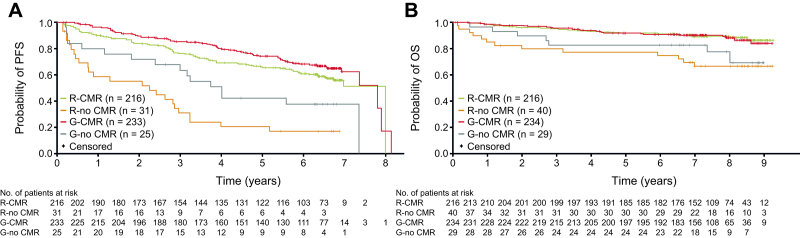
The phase III GALLIUM trial assessed the safety and efficacy of obinutuzumab-based versus rituximab-based immunochemotherapy in patients with previously untreated follicular lymphoma (FL) or marginal zone lymphoma (MZL). At the primary analysis, the trial met its primary end point, demonstrating improvement in investigator-assessed progression-free survival (PFS) with obinutuzumab-based versus rituximab-based immunochemotherapy in patients with FL. We report the results of the final analysis in the FL population, with an additional exploratory analysis in the MZL subgroup. Overall, 1202 patients with FL were randomized 1:1 to obinutuzumab- or rituximab-based immunochemotherapy followed by maintenance with the same antibody for up to 2 years. After a median 7.9 (range, 0.0-9.8) years of follow-up, PFS remained improved with obinutuzumab- versus rituximab-based immunochemotherapy, with 7-year PFS rates of 63.4% versus 55.7% (P = 0.006). Time-to-next antilymphoma treatment was also improved (74.1% versus 65.4% of patients had not started their next antilymphoma treatment at 7 y; P = 0.001). Overall survival was similar between the arms (88.5% versus 87.2%; P = 0.36). Irrespective of the treatment received, PFS and OS were higher in patients with a complete molecular response (CMR) versus those with no CMR (P < 0.001). Serious adverse events were reported in 48.9% and 43.4% of patients in the obinutuzumab and rituximab arms, respectively; there was no difference in the rate of fatal adverse events (4.4% and 4.5%, respectively). No new safety signals were reported. These data demonstrate the long-term benefit of obinutuzumab-based immunochemotherapy and confirm its role as a standard-of-care for the first-line treatment of advanced-stage FL, taking into account patient characteristics and safety considerations.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Hematology Association.
Conflict of interest statement
WT reports honoraria from F. Hoffmann-La Roche Ltd, Gilead Sciences, and Bristol-Myers Squibb, consultancy fees from F. Hoffmann-La Roche Ltd, Bristol-Myers Squibb, Incyte, and Takeda, and travel and conference registration fees from F. Hoffmann-La Roche Ltd, Gilead Sciences, and Takeda. WH reports honoraria from F. Hoffmann-La Roche Ltd, Janssen, Gilead Sciences and Celgene; a consulting/advisory role for F. Hoffmann-La Roche Ltd, Janssen and Gilead Sciences; speakers’ bureau for F. Hoffmann-La Roche Ltd, Janssen and Gilead Sciences; research funding from F. Hoffmann-La Roche Ltd, Janssen and Bayer; and travel expenses/accommodation from F. Hoffmann-La Roche Ltd, Janssen and Gilead Sciences. CB reports honoraria and speakers’ bureau fees from, and a consulting/advisory role for F. Hoffmann-La Roche Ltd, Pfizer, Janssen, Hexal, Celltrion Healthcare, AbbVie, Novartis, Bayer, MorphoSys, Regeneron Pharmaceuticals, and BeiGene; and research funding from F. Hoffmann-La Roche Ltd, Janssen, Celltrion Healthcare, AbbVie, Bayer, Amgen, and MSD. GC reports a consultancy role for F. Hoffmann-La Roche Ltd and Celgene; and honoraria from Bristol-Myers Squibb, Sanofi, Janssen, Gilead Sciences, AbbVie, Takeda, F. Hoffmann-La Roche Ltd, and Celgene. DC acknowledges support and funding from the Royal Marsden NIHR Biomedical Research Center. MJSD reports research funding from F. Hoffmann-La Roche Ltd. JGG reports grants and personal fees from Celgene, AstraZeneca and Janssen; and personal fees from AbbVie, Gilead, Karyopharm, MorphoSys, Novartis, and T.G. Therapeutics.EP reports speakers’ fees from Gilead Sciences, advisory board fees from BeiGene, virtual conference attendance fees from Celgene, and travel and conference registration fees from Takeda. MD reports research funding from AbbVie, Bayer, Bristol-Myers Squibb/Celgene, Gilead Sciences/Kite, Janssen, and F. Hoffmann-La Roche Ltd; honoraria from Amgen, AstraZeneca, Gilead Sciences/Kite, Janssen, Lilly, Novartis, and F. Hoffmann-La Roche Ltd; and membership on an entity’s Board of Directors or advisory committees for AstraZeneca, BeiGene, Bristol-Myers Squibb/Celgene, Gilead Sciences/Kite, Janssen, Lilly/Loxo Oncology, Novartis, and F. Hoffmann-La Roche Ltd. JFS reports speakers’ bureau fees, advisory board fees, and research funding from AbbVie, advisory board fees from AstraZeneca, advisory board fees from BeiGene, advisory board fees and research funding from Bristol-Myers Squibb, scientific advisory board membership from Genor Biopharma, advisory board fees from Gilead, advisory board fees and research funding from Janssen, advisory board fees, speakers’ bureau fees, research funding and expert testimony fees from F. Hoffmann-La Roche Ltd, and advisory and expert testimony fees from TG Therapeutics. JT reports research funding from F. Hoffmann-La Roche Ltd, Celgene, Janssen, PCYC, and BeiGene. DK, TGN, and AK is employed by and has equity ownership interests in F. Hoffmann-La Roche Ltd. MH reports a consultancy/advisory role with Celgene, Gilead, and F. Hoffmann-La Roche Ltd and research funding from F. Hoffmann-La Roche Ltd. RM reports honoraria from F. Hoffmann-La Roche Ltd and Janssen. All the other authors have no conflicts of interest to disclose.
Figures





References
-
- Freedman A, Jacobsen E. Follicular lymphoma: 2020 update on diagnosis and management. Am J Hematol. 2020;95:316–327. - PubMed
-
- Hiddemann W, Kneba M, Dreyling M, et al. Frontline therapy with rituximab added to the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) significantly improves the outcome for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: results of a prospective randomized study of the German Low-Grade Lymphoma Study Group. Blood. 2005;106:3725–3732. - PubMed
-
- Herold M, Haas A, Srock S, et al. Rituximab added to first-line mitoxantrone, chlorambucil, and prednisolone chemotherapy followed by interferon maintenance prolongs survival in patients with advanced follicular lymphoma: an East German Study Group Hematology and Oncology Study. J Clin Oncol. 2007;25:1986–1992. - PubMed
-
- Marcus R, Imrie K, Solal-Celigny P, et al. Phase III study of R-CVP compared with cyclophosphamide, vincristine, and prednisone alone in patients with previously untreated advanced follicular lymphoma. J Clin Oncol. 2008;26:4579–4586. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous