

Coronary Calcium Predicts All-Cause Mortality in Suspected Acute Aortic Syndrome
- PMID: 37404788
- PMCID: PMC10316301
- DOI: 10.1148/ryct.220188
Coronary Calcium Predicts All-Cause Mortality in Suspected Acute Aortic Syndrome
Abstract
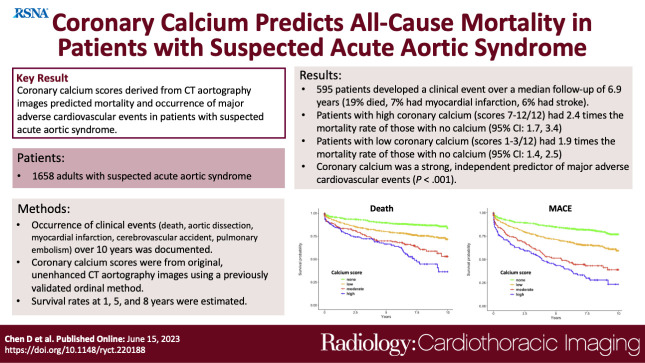
Purpose: To determine long-term clinical outcomes in patients with suspected acute aortic syndrome (AAS) and evaluate the prognostic value of coronary calcium burden as assessed with CT aortography in this symptomatic population.
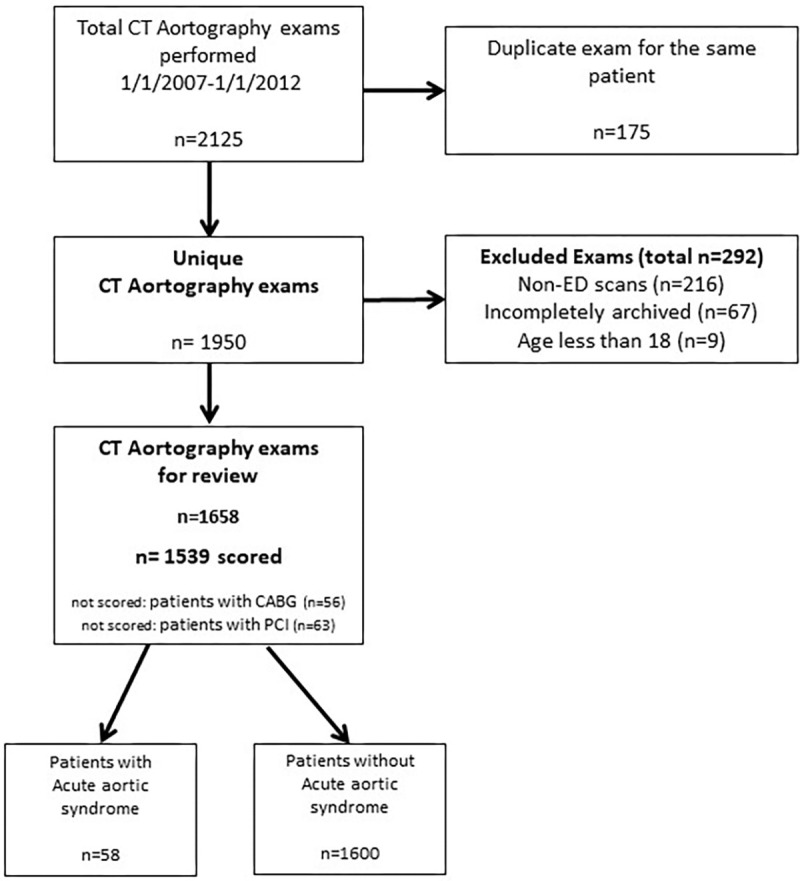
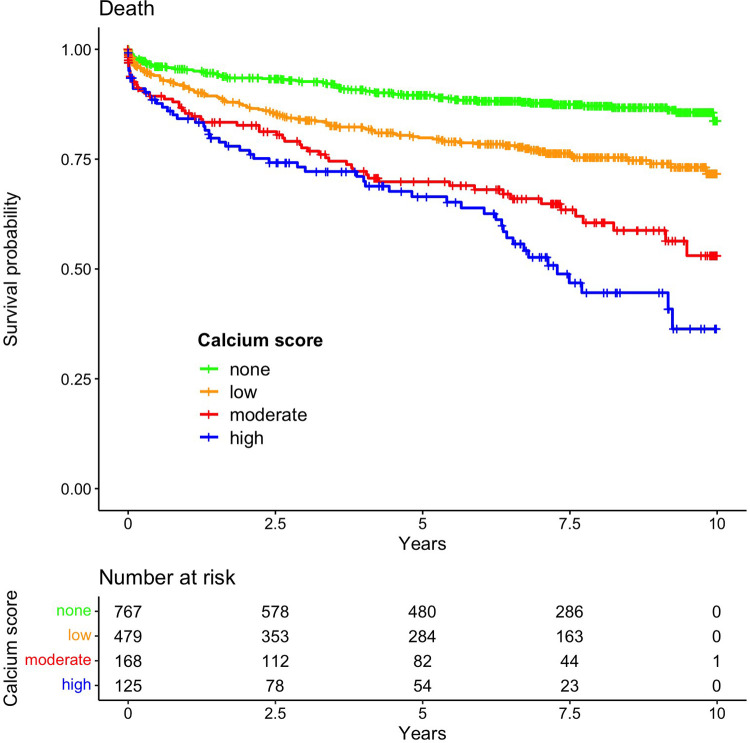
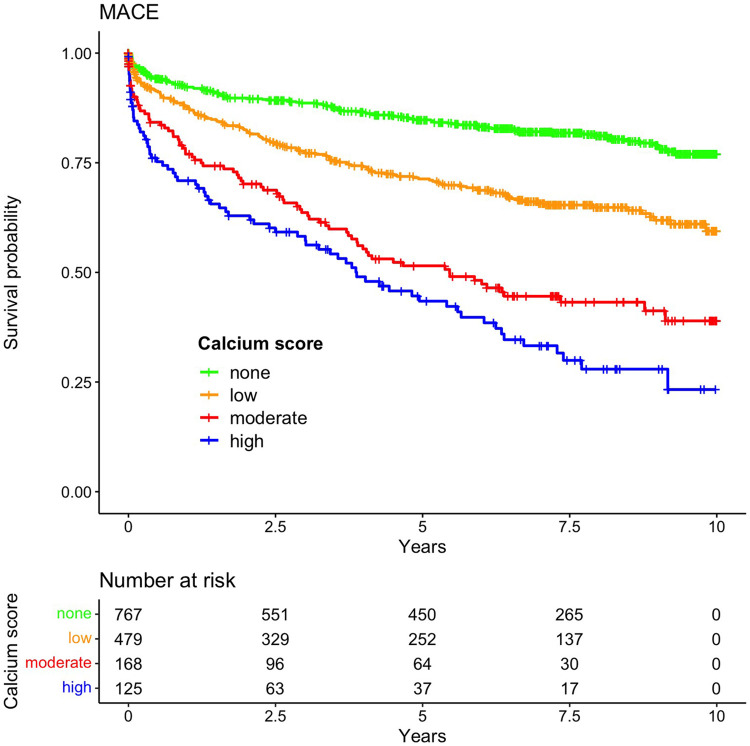
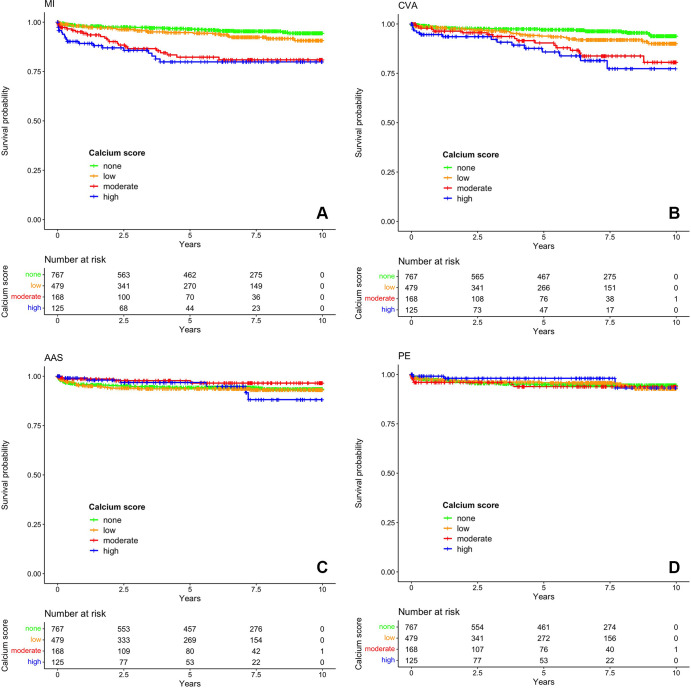
Materials and methods: A retrospective cohort of all patients who underwent emergency CT aortography from January 2007 through January 2012 for suspected AAS was assembled. A medical record survey tool was used to evaluate subsequent clinical events over 10 years of follow-up. Events included death, aortic dissection, myocardial infarction, cerebrovascular accident, and pulmonary embolism. Coronary calcium scores were computed from original images using a validated simple 12-point ordinal method and categorized into none, low (1-3), moderate (4-6), or high (7-12) groupings. Survival analysis with Kaplan-Meier curves and Cox proportional hazard modeling was performed.
Results: The study cohort comprised 1658 patients (mean age, 60 years ± 16 [SD]; 944 women), with 595 (35.9%) developing a clinical event over a median follow-up of 6.9 years. Patients with high coronary calcium demonstrated the highest mortality rate (adjusted hazard ratio = 2.36; 95% CI: 1.65, 3.37). Patients with low coronary calcium demonstrated lower mortality, but rates were still almost twice as high compared with patients with no detectable calcium (adjusted hazard ratio = 1.89; 95% CI: 1.41, 2.53). Coronary calcium was a strong predictor of major adverse cardiovascular events (P < .001), which persisted after adjustment for common significant comorbidities.
Conclusion: Patients with suspected AAS had a high rate of subsequent clinical events, including death. CT aortography-based coronary calcium scores strongly and independently predicted all-cause mortality.Keywords: Acute Aortic Syndrome, Coronary Artery Calcium, CT Aortography, Major Adverse Cardiovascular Events, Mortality Supplemental material is available for this article. © RSNA, 2023See also commentary by Weir-McCall and Shambrook in this issue.
Keywords: Acute Aortic Syndrome; CT Aortography; Coronary Artery Calcium; Major Adverse Cardiovascular Events; Mortality.
© 2023 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of conflicts of interest: D.C. No relevant relationships. A.R.S. No relevant relationships. K.Y. No relevant relationships. J.M.L. No relevant relationships.
Figures
Similar articles
-
Visually assessed coronary and cardiac calcium outperforms perfusion data during scintigraphy in the prediction of adverse outcomes.Int J Cardiol. 2020 Aug 1;312:123-128. doi: 10.1016/j.ijcard.2020.03.032. Epub 2020 Mar 12. Int J Cardiol. 2020. PMID: 32201100
-
Ethnic Disparities in CT Aortography Use for Diagnosing Acute Aortic Syndrome.Radiol Cardiothorac Imaging. 2022 Nov 17;4(6):e220018. doi: 10.1148/ryct.220018. eCollection 2022 Dec. Radiol Cardiothorac Imaging. 2022. PMID: 36601460 Free PMC article.
-
Beta-blockers for suspected or diagnosed acute myocardial infarction.Cochrane Database Syst Rev. 2019 Dec 17;12(12):CD012484. doi: 10.1002/14651858.CD012484.pub2. Cochrane Database Syst Rev. 2019. PMID: 31845756 Free PMC article.
-
Coronary CT Fractional Flow Reserve before Transcatheter Aortic Valve Replacement: Clinical Outcomes.Radiology. 2022 Jan;302(1):50-58. doi: 10.1148/radiol.2021210160. Epub 2021 Oct 5. Radiology. 2022. PMID: 34609200
-
The prognostic value of automated coronary calcium derived by a deep learning approach on non-ECG gated CT images from 82Rb-PET/CT myocardial perfusion imaging.Int J Cardiol. 2021 Apr 15;329:9-15. doi: 10.1016/j.ijcard.2020.12.079. Epub 2021 Jan 4. Int J Cardiol. 2021. PMID: 33412176
Cited by
-
CT in Suspected Acute Aortic Syndrome: An Opportunity for Improving Cardiovascular Outcomes?Radiol Cardiothorac Imaging. 2023 Jun 15;5(3):e230129. doi: 10.1148/ryct.230129. eCollection 2023 Jun. Radiol Cardiothorac Imaging. 2023. PMID: 37404784 Free PMC article. No abstract available.
-
Coronary Calcium Association with All-Cause Mortality in Suspected Acute Aortic Syndrome.Radiol Cardiothorac Imaging. 2023 Aug 31;5(4):e230171. doi: 10.1148/ryct.230171. eCollection 2023 Aug. Radiol Cardiothorac Imaging. 2023. PMID: 37693200 Free PMC article. No abstract available.
References
-
- Tsai TT , Nienaber CA , Eagle KA . Acute aortic syndromes . Circulation 2005. ; 112 ( 24 ): 3802 – 3813 . - PubMed
-
- Pape LA , Awais M , Woznicki EM , et al. . Presentation, diagnosis, and outcomes of acute aortic dissection: 17-year trends from the International Registry of Acute Aortic Dissection . J Am Coll Cardiol 2015. ; 66 ( 4 ): 350 – 358 . - PubMed
-
- Wnorowski AM , Halpern EJ . Diagnostic yield of triple-rule-out CT in an emergency setting . AJR Am J Roentgenol 2016. ; 207 ( 2 ): 295 – 301 . - PubMed
LinkOut - more resources
Full Text Sources
