

Ability of lactulose breath test results to accurately identify colorectal polyps through the measurement of small intestine bacterial overgrowth
- PMID: 37405104
- PMCID: PMC10315122
- DOI: 10.4240/wjgs.v15.i6.1138
Ability of lactulose breath test results to accurately identify colorectal polyps through the measurement of small intestine bacterial overgrowth
Abstract
Background: While colorectal polyps are not cancerous, some types of polyps, known as adenomas, can develop into colorectal cancer over time. Polyps can often be found and removed by colonoscopy; however, this is an invasive and expensive test. Thus, there is a need for new methods of screening patients at high risk of developing polyps.
Aim: To identify a potential association between colorectal polyps and small intestine bacteria overgrowth (SIBO) or other relevant factors in a patient cohort with lactulose breath test (LBT) results.
Methods: A total of 382 patients who had received an LBT were classified into polyp and non-polyp groups that were confirmed by colonoscopy and pathology. SIBO was diagnosed by measuring LBT-derived hydrogen (H) and methane (M) levels according to 2017 North American Consensus recommendations. Logistic regression was used to assess the ability of LBT to predict colorectal polyps. Intestinal barrier function damage (IBFD) was determined by blood assays.
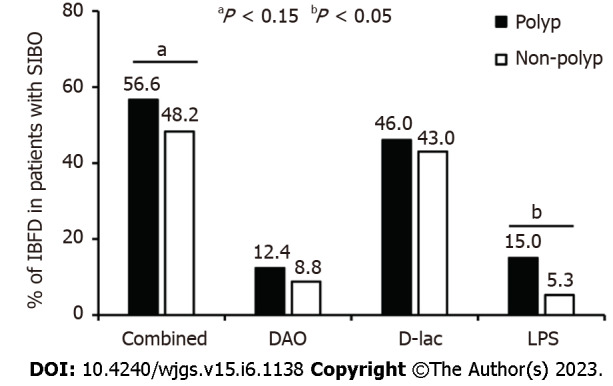
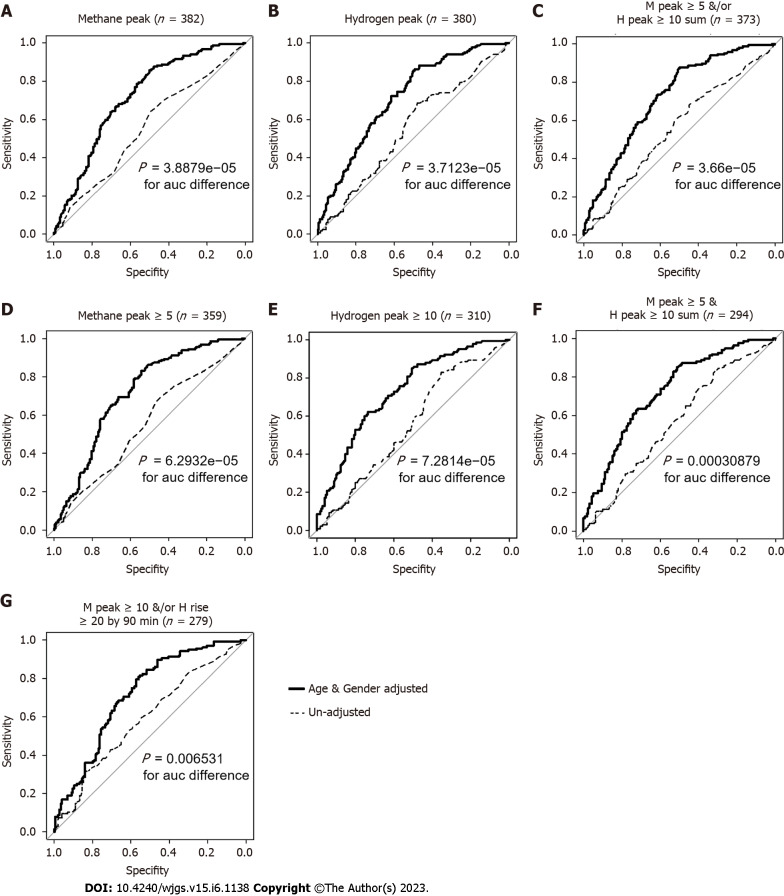
Results: H and M levels revealed that the prevalence of SIBO was significantly higher in the polyp group than in the non-polyp group (41% vs 23%, P < 0.01; 71% vs 59%, P < 0.05, respectively). Within 90 min of lactulose ingestion, the peak H values in the adenomatous and inflammatory/hyperplastic polyp patients were significantly higher than those in the non-polyp group (P < 0.01, and P = 0.03, respectively). In 227 patients with SIBO defined by combining H and M values, the rate of IBFD determined by blood lipopolysaccharide levels was significantly higher among patients with polyps than those without (15% vs 5%, P < 0.05). In regression analysis with age and gender adjustment, colorectal polyps were most accurately predicted with models using M peak values or combined H and M values limited by North American Consensus recommendations for SIBO. These models had a sensitivity of ≥ 0.67, a specificity of ≥ 0.64, and an accuracy of ≥ 0.66.
Conclusion: The current study made key associations among colorectal polyps, SIBO, and IBFD and demonstrated that LBT has moderate potential as an alternative noninvasive screening tool for colorectal polyps.
Keywords: Colorectal polyp; Intestinal barrier function; Lactulose breath test; Retrospective study; Small intestine bacteria overgrowth.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare. There are no ethical or legal conflicts involved in the article.
Figures
Similar articles
-
[Clinical features of irritable bowel syndrome with small intestinal bacterial overgrowth and a preliminary study of effectiveness of Rifaximin].Zhonghua Yi Xue Za Zhi. 2016 Jun 28;96(24):1896-902. doi: 10.3760/cma.j.issn.0376-2491.2016.24.005. Zhonghua Yi Xue Za Zhi. 2016. PMID: 27373356 Chinese.
-
Elevated methane levels in small intestinal bacterial overgrowth suggests delayed small bowel and colonic transit.Medicine (Baltimore). 2018 May;97(21):e10554. doi: 10.1097/MD.0000000000010554. Medicine (Baltimore). 2018. PMID: 29794732 Free PMC article.
-
Impact of Oral-Cecal Transit Time on the Interpretation of Lactulose Breath Tests After RYGB: a Personalized Approach to the Diagnosis of SIBO.Obes Surg. 2019 Mar;29(3):771-775. doi: 10.1007/s11695-018-3575-3. Obes Surg. 2019. PMID: 30627990
-
Breath testing for small intestinal bacterial overgrowth: maximizing test accuracy.Clin Gastroenterol Hepatol. 2014 Dec;12(12):1964-72; quiz e119-20. doi: 10.1016/j.cgh.2013.09.055. Epub 2013 Oct 1. Clin Gastroenterol Hepatol. 2014. PMID: 24095975 Review.
-
Association of small intestinal bacterial overgrowth with Parkinson's disease: a systematic review and meta-analysis.Gut Pathog. 2021 Apr 16;13(1):25. doi: 10.1186/s13099-021-00420-w. Gut Pathog. 2021. PMID: 33863370 Free PMC article. Review.
Cited by
-
Molecular Hydrogen Therapy: Mechanisms, Delivery Methods, Preventive, and Therapeutic Application.MedComm (2020). 2025 Apr 28;6(5):e70194. doi: 10.1002/mco2.70194. eCollection 2025 May. MedComm (2020). 2025. PMID: 40297245 Free PMC article. Review.
-
The Lactulose Breath Test Can Predict Refractory Gastroesophageal Reflux Disease by Measuring Bacterial Overgrowth in the Small Intestine.J Clin Gastroenterol. 2025 May-Jun 01;59(5):448-455. doi: 10.1097/MCG.0000000000002031. Epub 2024 Jun 13. J Clin Gastroenterol. 2025. PMID: 38896424 Free PMC article.
-
Causal Relationship Between Gut Microbiota and Gastrointestinal Polyps: A Mendelian Randomization Study.Turk J Gastroenterol. 2025 Jan 6;36(5):302-311. doi: 10.5152/tjg.2025.24347. Turk J Gastroenterol. 2025. PMID: 40241582 Free PMC article.
References
-
- Chinese Society of Gastroenterology, Cancer Collaboration Group of Chinese Society of Gastroenterology, Chinese Medical Association. Chinese consensus on prevention of colorectal neoplasia (2021, Shanghai) J Dig Dis . 2022;23:58–90. - PubMed
-
- Bretthauer M, Kalager M, Adami HO. Do's and don'ts in evaluation of endoscopic screening for gastrointestinal cancers. Endoscopy . 2016;48:75–80. - PubMed
-
- Øines M, Helsingen LM, Bretthauer M, Emilsson L. Epidemiology and risk factors of colorectal polyps. Best Pract Res Clin Gastroenterol . 2017;31:419–424. - PubMed
-
- Hikino K, Koido M, Otomo N, Tomizuka K, Ikegawa S, Matsuda K, Momozawa Y Biobank Japan Project, Mushiroda T, Terao C. Genome-wide association study of colorectal polyps identified highly overlapping polygenic architecture with colorectal cancer. J Hum Genet . 2022;67:149–156. - PubMed
LinkOut - more resources
Full Text Sources
