

Phenotypical Variability of the Internal Acoustic Canal in the Middle Cranial Fossa Surgery
- PMID: 37405241
- PMCID: PMC10317566
- DOI: 10.1055/a-1786-9026
Phenotypical Variability of the Internal Acoustic Canal in the Middle Cranial Fossa Surgery
Abstract
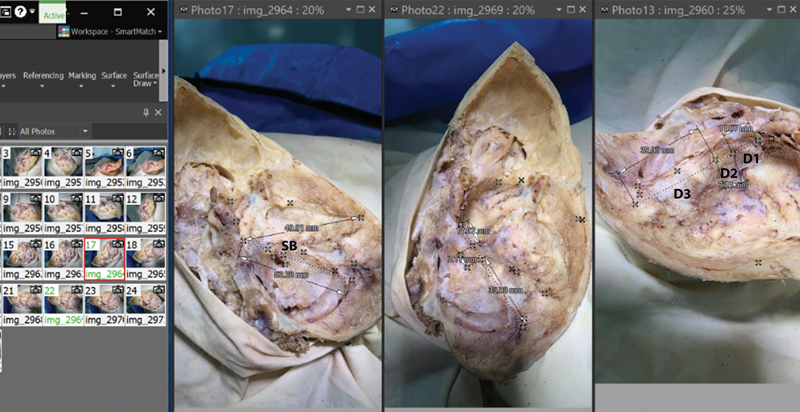
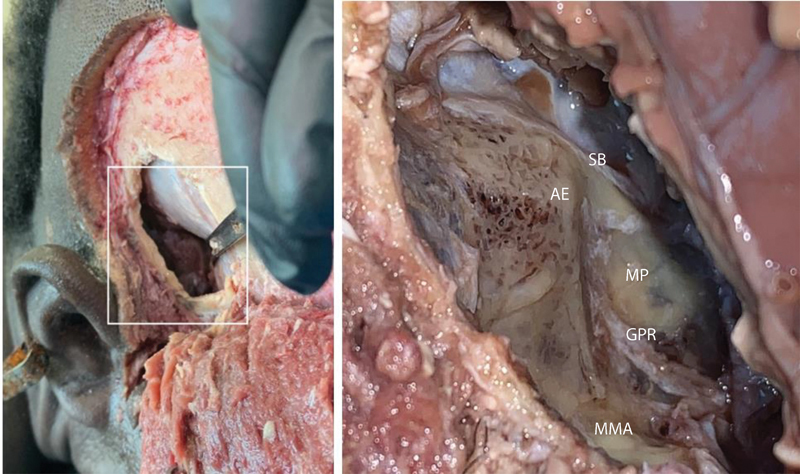
Introduction The wide range of anatomical variability of the structures of the middle cranial fossa (MCF) and the lack of reliable surgical landmarks contribute to a high level of complications in the surgical treatment of vestibular schwannomas. We hypothesized that the cranial phenotype influences the shape of the MCF, the orientation of the pyramid of the temporal bone, and the relative topography of the internal acoustic canal (IAC). Methods The skull base structures were studied on 54 embalmed cadavers and 60 magnetic resonance images of the head and neck by photo modeling, dissection, and three-dimensional analysis techniques. By the value of the cranial index, all specimens were subdivided into dolichocephalic, mesocephalic, and brachycephalic groups for comparison of variables. Results The length of the superior border of the temporal pyramid (SB), the apex to squama distance, and the width of the MCF all peaked in the brachycephalic group. The value of the angle between the SB and the axis of the acoustic canal varied from 33 to 58 degrees; it peaked in the dolichocephalic group and showed its smaller value in the brachycephalic one. The pyramid to squama angle had reversed distribution and dominated in the brachycephalic group. Conclusion The cranial phenotype influences the shape of the MCF, temporal pyramid, and IAC. Presented in this article data help specialists operating on the vestibular schwannoma to localize the IAC based on the individual shape of a skull.
Keywords: anatomical variability; cranial index; internal acoustic canal; middle cranial fossa; temporal bone; vestibular schwannoma.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures






References
-
- Myrseth E, Pedersen P H, Møller P, Lund-Johansen M.Treatment of vestibular schwannomas. Why, when and how? Acta Neurochir (Wien) 200714907647–660., discussion 660 - PubMed
-
- Gonzalez F, Ferreira M, Zabramski J, Spetzler R, Deshmukh P. The middle fossa approach. Barrow Quarterly. 2000;16(04):67–85.
-
- Staecker H, Nadol J B, Jr, Ojeman R, Ronner S, McKenna M J. Hearing preservation in acoustic neuroma surgery: middle fossa versus retrosigmoid approach. Am J Otol. 2000;21(03):399–404. - PubMed
-
- Farahani R, Nooranipour M, Nikakhtar K. Anthropometry of internal acoustic meatus. Int J Morphol. 2007;5(04):861–865.
-
- Faure A, Masse H, Gayet-Delacroix M. What is the arcuate eminence? Surg Radiol Anat. 2003;25(02):99–104. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous