

Fatal intracranial haemorrhage in acute promyelocytic leukemia patients with short isoform of PML-RARα: Review of molecular and radiological data
- PMID: 37405260
- PMCID: PMC10316003
- DOI: 10.1016/j.sjbs.2023.103710
Fatal intracranial haemorrhage in acute promyelocytic leukemia patients with short isoform of PML-RARα: Review of molecular and radiological data
Abstract
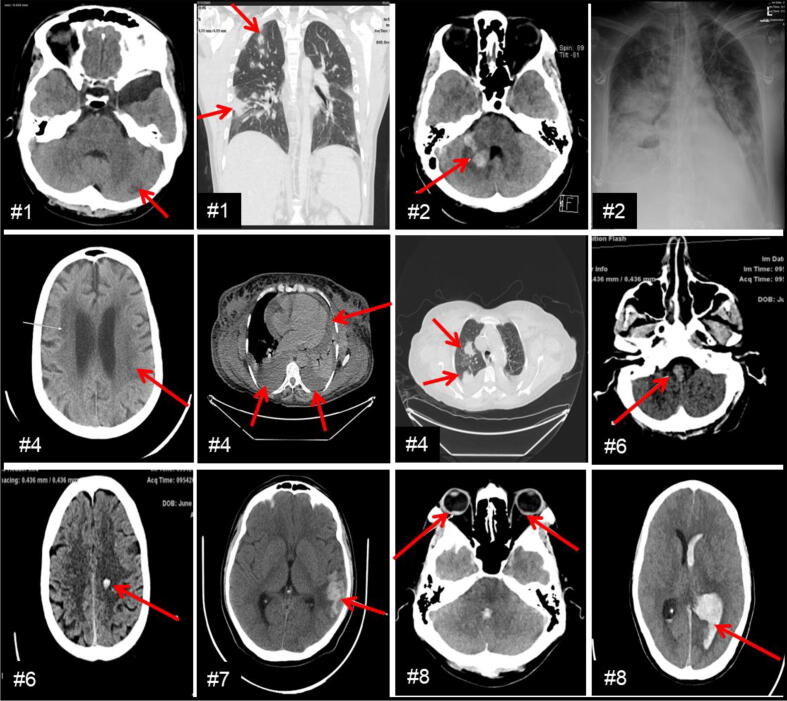
Three major PML-RARα fusion gene transcripts (long [bcr1], variant [bcr2], and short [bcr3]) are currently used in clinical laboratories for the diagnosis and treatment monitoring of APL patients. Despite highly improved outcome, relapse and intracranial haemorrhage that may lead to early death is still an unsolved complication in APL. We reviewed APL patients confirmed by qPCR for the presence of PML-RARα transcripts (n = 27) and studied their outcome in relation to the isoform expression at diagnosis and follow-up in King Fahad Medical City. Eight in twenty-seven patients showed bcr3 and nineteen patients with bcr1 as major isoforms at diagnosis. Half of the bcr3 patients (n = 4/8) showed early mortality, prolonged qPCR positivity, 4-fold higher neutrophil/lymphocyte ratio, higher creatinine levels, and significantly reduced relapse free and overall survival time compared with bcr1 patients. Radiological findings in bcr3 patients revealed CNS involvement in the form of intracranial haemorrhage and periventricular microangiopathy and no CNS involvement in bcr1 patients. In conclusion, PML-RARα isoform expression at diagnosis in selective patients influences disease course over time and may even lead to early mortality due to haemorrhage. Thus, timely reporting of the specific PML-RARα isoform by clinical laboratories and CNS assessment by radiology can prevent complications leading to death in some APL patients.
Keywords: Acute promyelocytic leukemia (APL); All-trans-retinoic acid (ATRA); Arsenic trioxide (ATO); Central nervous system (CNS); Computerized tomography (CT); Minimal residual disease (MRD); Molecular remission (MR); PML-RARα isoforms; Quantitative polymerase chain reaction (qPCR).
© 2023 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
-
- Abaza Y., Kantarjian H., Garcia-Manero G., Estey E., Borthakur G., Jabbour E., Faderl S., O’Brien S., Wierda W., Pierce S., Brandt M., McCue D., Luthra R., et al. Long-term outcome of acute promyelocytic leukemia treated with all-trans-retinoic acid, arsenic trioxide, and gemtuzumab. Blood. 2017;129:1275–1283. doi: 10.1182/blood-2016-09-736686. - DOI - PMC - PubMed
-
- De Botton S., Dombret H., Sanz M., Miguel J.S., Caillot D., Zittoun R., Gardembas M., Stamatoulas A., Condé E., Guerci A., Gardin C., Geiser K., Makhoul D.C., Reman O., de la Serna J., Lefrere F., Chomienne C., Chastang C., Degos L., Fenaux P. Incidence, clinical features, and outcome of all trans-retinoic acid syndrome in 413 cases of newly diagnosed acute promyelocytic leukemia. The European APL Group. Blood. 1998;15;92(8):2712–8 - PubMed
-
- De Thé H., Chomienne C., Lanotte M., Degos L., Dejean A. The t(15;17) translocation of acute promyelocytic leukaemia fuses the retinoic acid receptor α gene to a novel transcribed locus. Nature. 1990;347:558–561. - PubMed
LinkOut - more resources
Full Text Sources
