

Mid-Activity and At-Home Wearable Bioimpedance Elucidates an Interpretable Digital Biomarker of Muscle Fatigue
- PMID: 37405890
- PMCID: PMC11092386
- DOI: 10.1109/TBME.2023.3290530
Mid-Activity and At-Home Wearable Bioimpedance Elucidates an Interpretable Digital Biomarker of Muscle Fatigue
Abstract
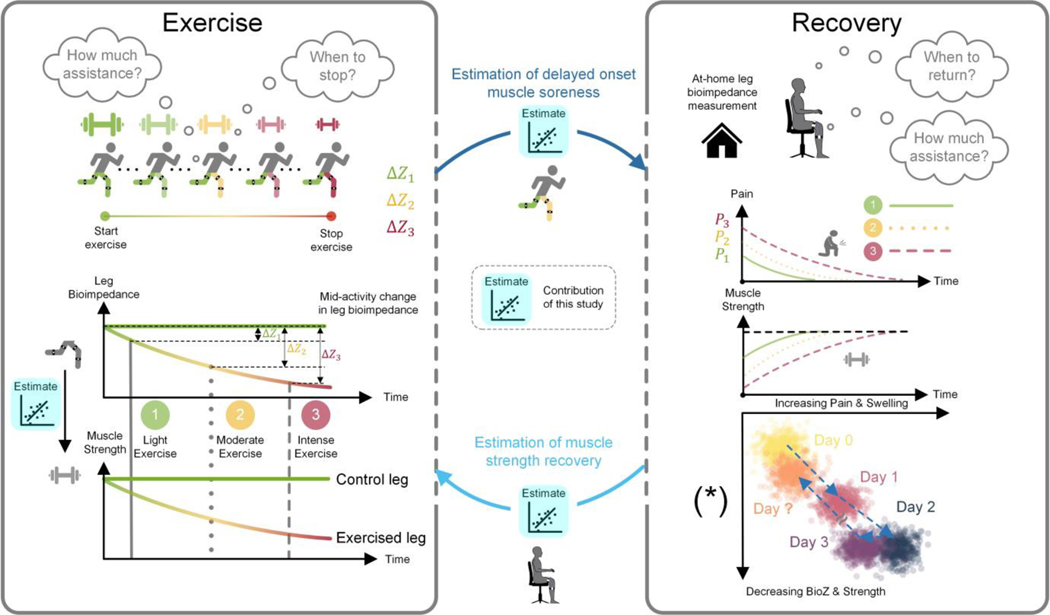
Objective: Muscle health and decreased muscle performance (fatigue) quantification has proven to be an invaluable tool for both athletic performance assessment and injury prevention. However, existing methods estimating muscle fatigue are infeasible for everyday use. Wearable technologies are feasible for everyday use and can enable discovery of digital biomarkers of muscle fatigue. Unfortunately, the current state-of-the-art wearable systems for muscle fatigue tracking suffer from either low specificity or poor usability.
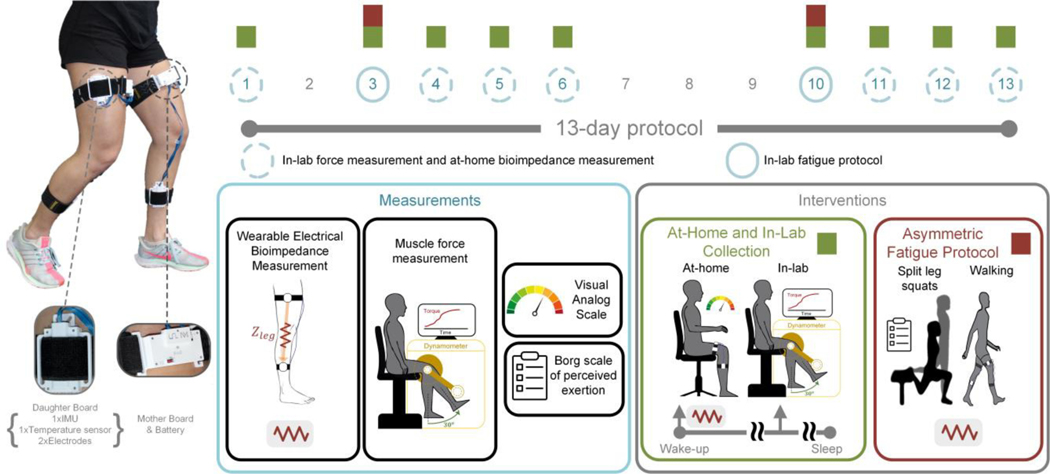
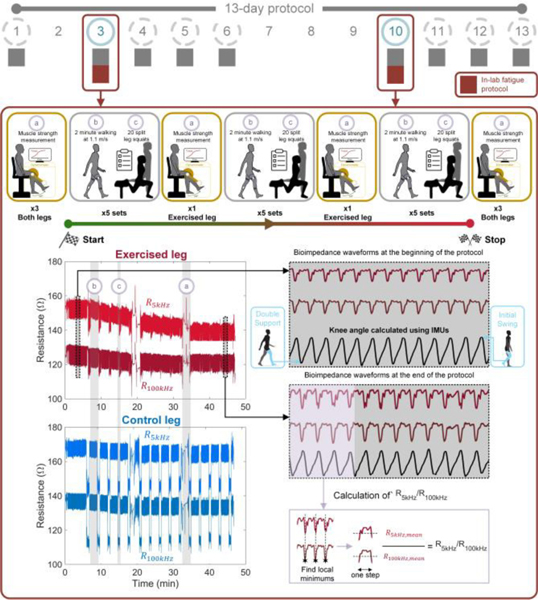
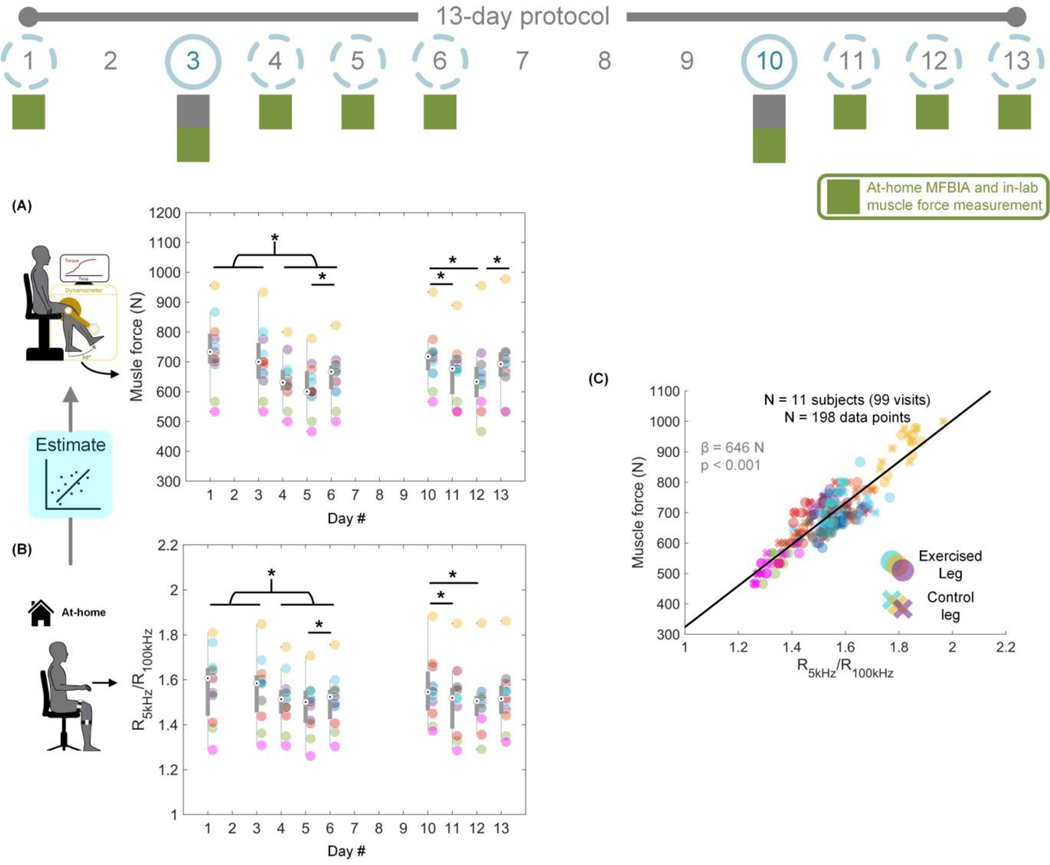
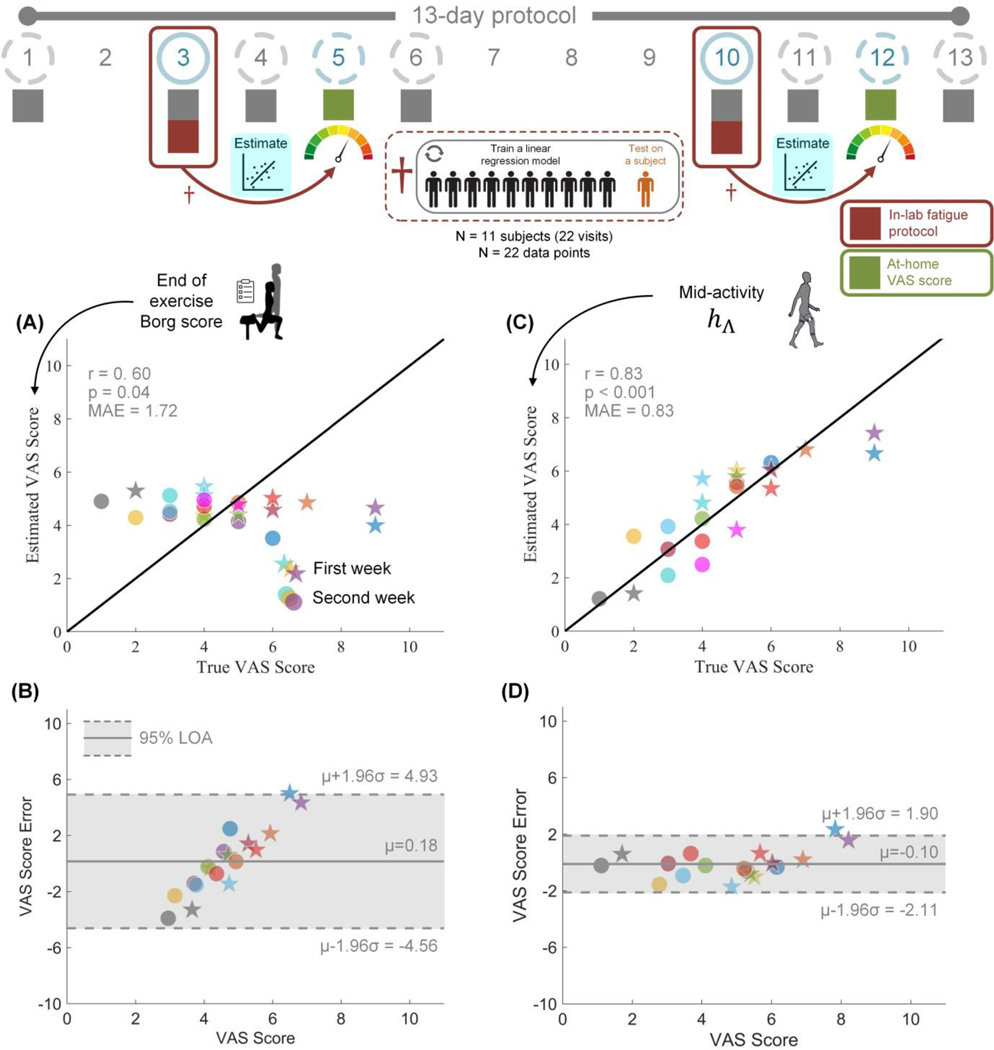
Methods: We propose using dual-frequency bioimpedance analysis (DFBIA) to non-invasively assess intramuscular fluid dynamics and thereby muscle fatigue. A wearable DFBIA system was developed to measure leg muscle fatigue of 11 individuals during a 13-day protocol consisting of exercise and unsupervised at-home portions.
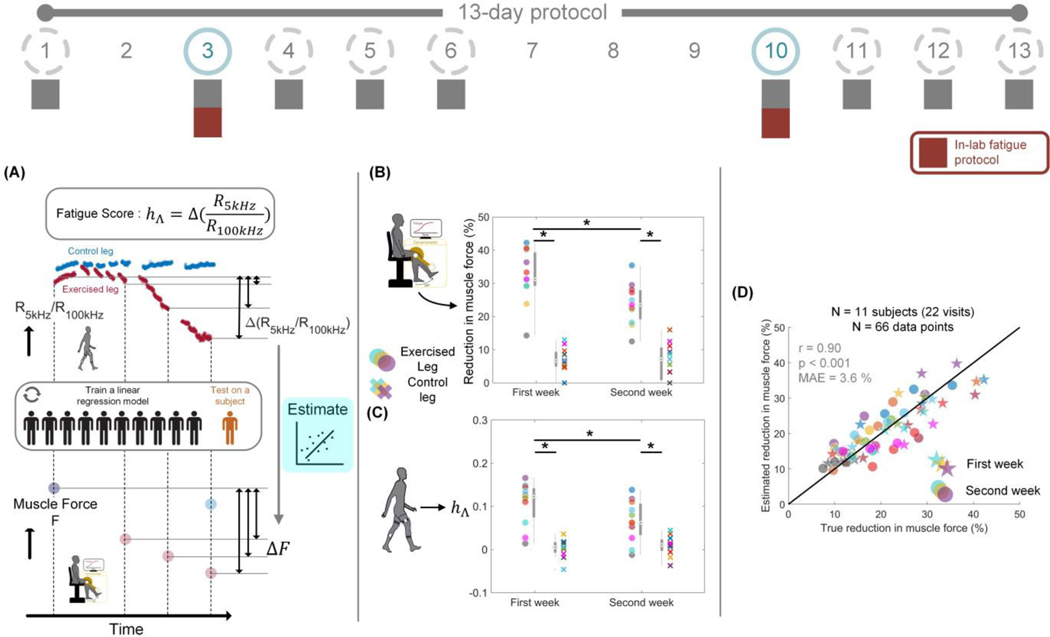
Results: We derived a digital biomarker of muscle fatigue, fatigue score, from the DFBIA signals that was able to estimate the percent reduction in muscle force during exercise with repeated-measures Pearson's r = 0.90 and mean absolute error (MAE) of 3.6%. This fatigue score also estimated delayed onset muscle soreness with repeated-measures Pearson's r = 0.83 and MAE = 0.83. Using at-home data, DFBIA was strongly associated with absolute muscle force of participants (n = 198, p < 0.001).
Conclusion: These results demonstrate the utility of wearable DFBIA for non-invasively estimating muscle force and pain through the changes in intramuscular fluid dynamics.
Significance: The presented approach may inform development of future wearable systems for quantifying muscle health and provide a novel framework for athletic performance optimization and injury prevention.
Figures
Similar articles
-
Effectiveness of Using a Digital Wearable Plantar Pressure Device to Detect Muscle Fatigue: Within-Subject, Repeated Measures Experimental Design.JMIR Hum Factors. 2025 Jan 7;12:e65578. doi: 10.2196/65578. JMIR Hum Factors. 2025. PMID: 39773695 Free PMC article.
-
Wearable Mid-Activity Measurement of Lower Limb Electrical Bioimpedance Estimates Vertical Ground Reaction Force Features.Annu Int Conf IEEE Eng Med Biol Soc. 2022 Jul;2022:91-94. doi: 10.1109/EMBC48229.2022.9871267. Annu Int Conf IEEE Eng Med Biol Soc. 2022. PMID: 36085606
-
Investigating Changes in Muscle Coordination During Cycling with Soft Wearable Strain Sensors Sensitive to Muscle Deformation.IEEE Int Conf Rehabil Robot. 2023 Sep;2023:1-6. doi: 10.1109/ICORR58425.2023.10304718. IEEE Int Conf Rehabil Robot. 2023. PMID: 37941290
-
Neuromuscular fatigue during repeated sprint exercise: underlying physiology and methodological considerations.Appl Physiol Nutr Metab. 2018 Nov;43(11):1166-1175. doi: 10.1139/apnm-2018-0080. Epub 2018 Apr 27. Appl Physiol Nutr Metab. 2018. PMID: 29701482 Review.
-
The stretch-shortening cycle : a model to study naturally occurring neuromuscular fatigue.Sports Med. 2006;36(11):977-99. doi: 10.2165/00007256-200636110-00004. Sports Med. 2006. PMID: 17052133 Review.
References
-
- “2018 Physical Activity Guidelines Advisory Committee Scientific Report,” p. 779.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
