

Starting at the community: Treatment-seeking pathways of children with suspected severe malaria in Uganda
- PMID: 37405978
- PMCID: PMC10321646
- DOI: 10.1371/journal.pgph.0001949
Starting at the community: Treatment-seeking pathways of children with suspected severe malaria in Uganda
Abstract
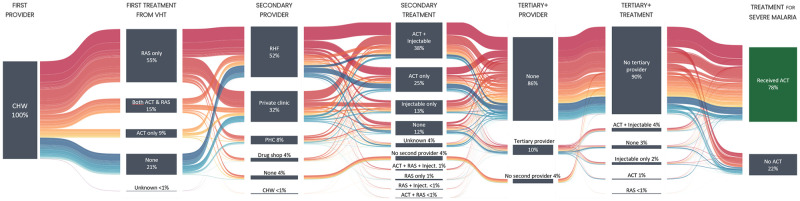
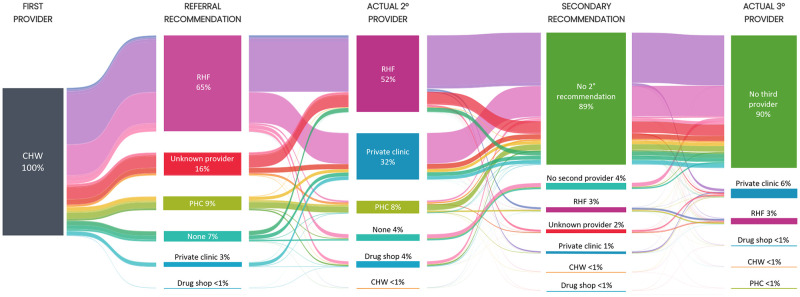
Community health workers (CHW) usually refer children with suspected severe malaria to the nearest public health facility or a designated public referral health facility (RHF). Caregivers do not always follow this recommendation. This study aimed at identifying post-referral treatment-seeking pathways that lead to appropriate antimalarial treatment for children less than five years with suspected severe malaria. An observational study in Uganda enrolled children below five years presenting to CHWs with signs of severe malaria. Children were followed up 28 days after enrolment to assess their condition and treatment-seeking history, including referral advice and provision of antimalarial treatment from visited providers. Of 2211 children included in the analysis, 96% visited a second provider after attending a CHW. The majority of CHWs recommended caregivers to take their child to a designated RHF (65%); however, only 59% followed this recommendation. Many children were brought to a private clinic (33%), even though CHWs rarely recommended this type of provider (3%). Children who were brought to a private clinic were more likely to receive an injection than children brought to a RHF (78% vs 51%, p<0.001) and more likely to receive the second or third-line injectable antimalarial (artemether: 22% vs. 2%, p<0.001, quinine: 12% vs. 3%, p<0.001). Children who only went to non-RHF providers were less likely to receive an artemisinin-based combination therapy (ACT) than children who attended a RHF (odds ratio [OR] = 0.64, 95% CI 0.51-0.79, p<0.001). Children who did not go to any provider after seeing a CHW were the least likely to receive an ACT (OR = 0.21, 95% CI 0.14-0.34, p<0.001). Health policies should recognise local treatment-seeking practices and ensure adequate quality of care at the various public and private sector providers where caregivers of children with suspected severe malaria actually seek care.
Copyright: © 2023 Brunner et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Young M, Wolfheim C, Marsh DR, Hammamy D. World Health Organization/United Nations Children’s Fund joint statement on integrated community case management: an equity-focused strategy to improve access to essential treatment services for children. Am J Trop Med Hyg. 2012;87(5 Suppl):6–10. doi: 10.4269/ajtmh.2012.12-0221 - DOI - PMC - PubMed
-
- Medicines for Malaria Venture. Artesunate rectal capsules tool kit 2016 [24.10.2021]. https://www.mmv.org/sites/default/files/uploads/docs/access/Rectal_artes....
LinkOut - more resources
Full Text Sources