

The effect of preoperative behaviour change interventions on pre- and post-surgery health behaviours, health outcomes, and health inequalities in adults: A systematic review and meta-analyses
- PMID: 37406002
- PMCID: PMC10321619
- DOI: 10.1371/journal.pone.0286757
The effect of preoperative behaviour change interventions on pre- and post-surgery health behaviours, health outcomes, and health inequalities in adults: A systematic review and meta-analyses
Abstract
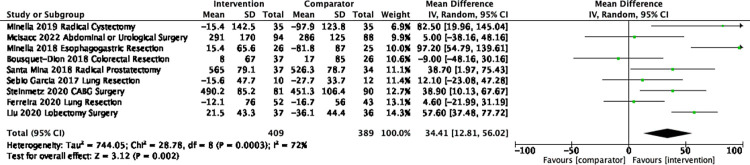
Background: Prehabilitation interventions are being delivered across surgical specialities to improve health risk behaviours leading to better surgical outcomes and potentially reduce length of hospital stay. Most previous research has focused on specific surgery specialities and has not considered the impact of interventions on health inequalities, nor whether prehabilitation improves health behaviour risk profiles beyond surgery. The aim of this review was to examine behavioural Prehabilitation interventions across surgeries to inform policy makers and commissioners of the best available evidence.
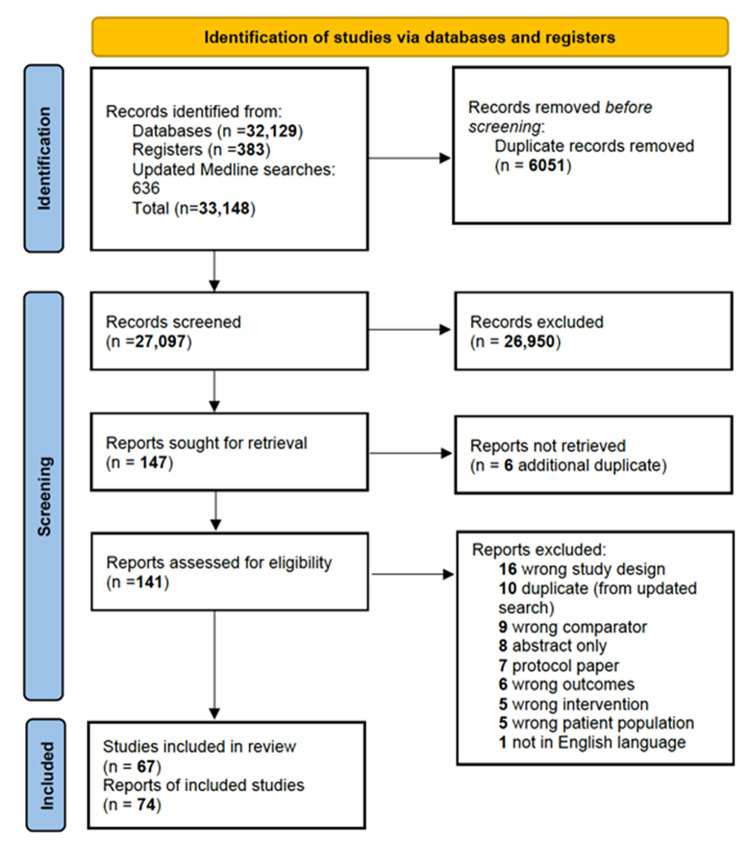
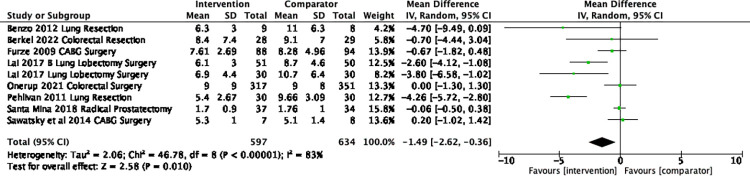
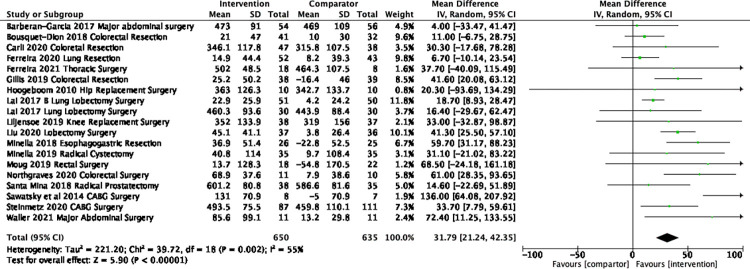
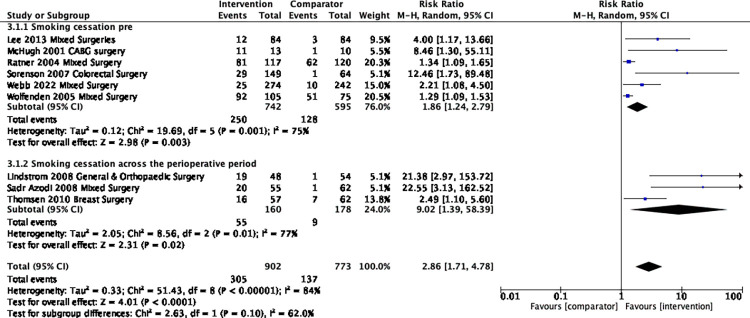
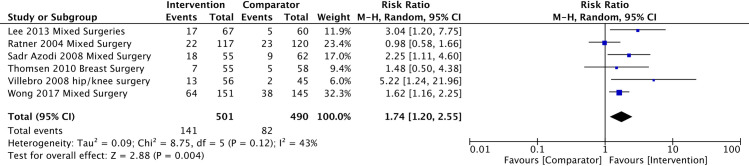
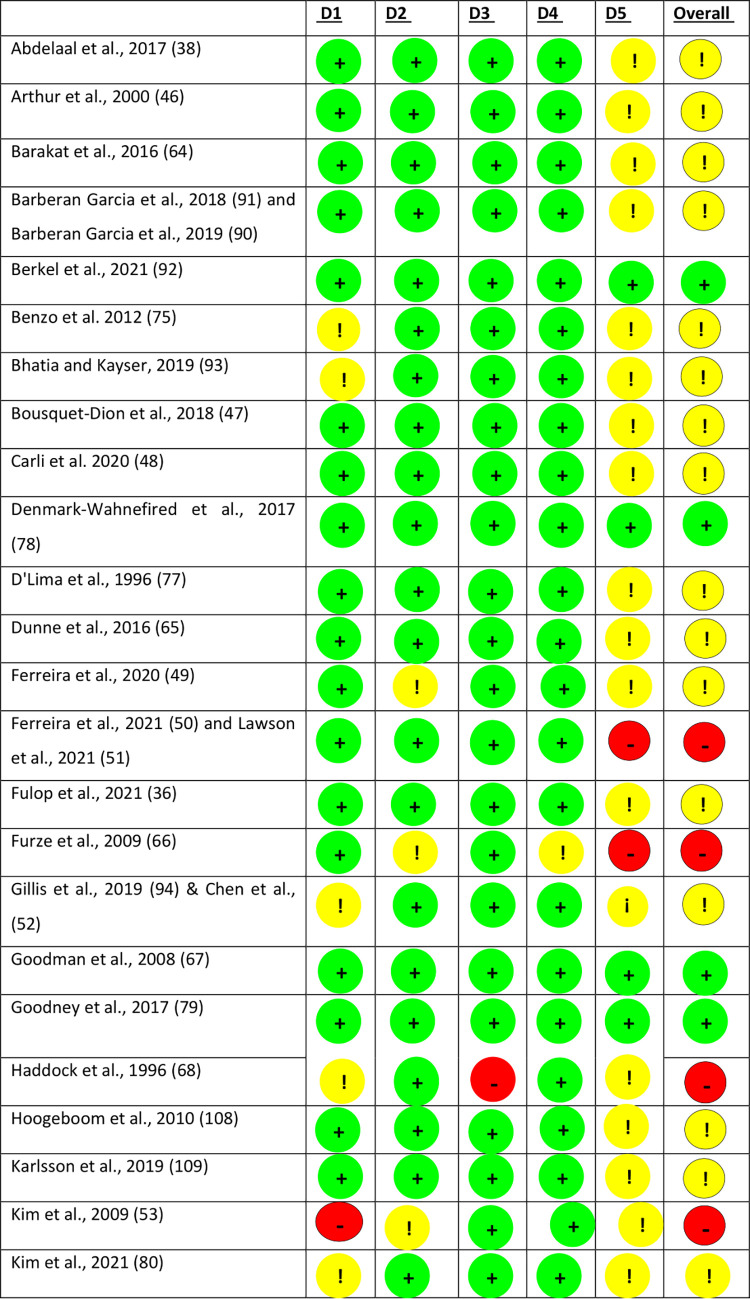
Methods and findings: A systematic review and meta-analysis of randomised controlled trials (RCTs) was conducted to determine the effect of behavioural prehabilitation interventions targeting at least one of: smoking behaviour, alcohol use, physical activity, dietary intake (including weight loss interventions) on pre- and post-surgery health behaviours, health outcomes, and health inequalities. The comparator was usual care or no treatment. MEDLINE, PubMed, PsychINFO, CINAHL, Web of Science, Google Scholar, Clinical trials and Embase databases were searched from inception to May 2021, and the MEDLINE search was updated twice, most recently in March 2023. Two reviewers independently identified eligible studies, extracted data, and assessed risk of bias using the Cochrane risk of bias tool. Outcomes were length of stay, six-minute walk test, behaviours (smoking, diet, physical activity, weight change, and alcohol), and quality of life. Sixty-seven trials were included; 49 interventions targeted a single behaviour and 18 targeted multiple behaviours. No trials examined effects by equality measures. Length of stay in the intervention group was 1.5 days shorter than the comparator (n = 9 trials, 95% CI -2.6 to -0.4, p = 0.01, I2 83%), although in sensitivity analysis prehabilitation had the most impact in lung cancer patients (-3.5 days). Pre-surgery, there was a mean difference of 31.8 m in the six-minute walk test favouring the prehabilitation group (n = 19 trials, 95% CI 21.2 to 42.4m, I2 55%, P <0.001) and this was sustained to 4-weeks post-surgery (n = 9 trials, mean difference = 34.4m (95%CI 12.8 to 56.0, I2 72%, P = 0.002)). Smoking cessation was greater in the prehabilitation group before surgery (RR 2.9, 95% CI 1.7 to 4.8, I2 84%), and this was sustained at 12 months post-surgery (RR 1.74 (95% CI 1.20 to 2.55, I2 43%, Tau2 0.09, p = 0.004)There was no difference in pre-surgery quality of life (n = 12 trials) or BMI (n = 4 trials).
Conclusions: Behavioural prehabilitation interventions reduced length of stay by 1.5 days, although in sensitivity analysis the difference was only found for Prehabilitation interventions for lung cancer. Prehabilitation can improve functional capacity and smoking outcomes just before surgery. That improvements in smoking outcomes were sustained at 12-months post-surgery suggests that the surgical encounter holds promise as a teachable moment for longer-term behavioural change. Given the paucity of data on the effects on other behavioural risk factors, more research grounded in behavioural science and with longer-term follow-up is needed to further investigate this potential.
Copyright: © 2023 Fong et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
No authors have competing interest.
Figures
References
-
- Organisation for Economic Co-operation and Development (OECD). Waiting times 2020. [Available from: https://www.oecd.org/els/health-systems/waiting-times.htm.
-
- NHS England. Delivery plan for tackling the COVID-19 backlog of elective care. 2022. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
