

Artificial Intelligence Application to Screen Abdominal Aortic Aneurysm Using Computed tomography Angiography
- PMID: 37407843
- PMCID: PMC10501994
- DOI: 10.1007/s10278-023-00866-1
Artificial Intelligence Application to Screen Abdominal Aortic Aneurysm Using Computed tomography Angiography
Abstract
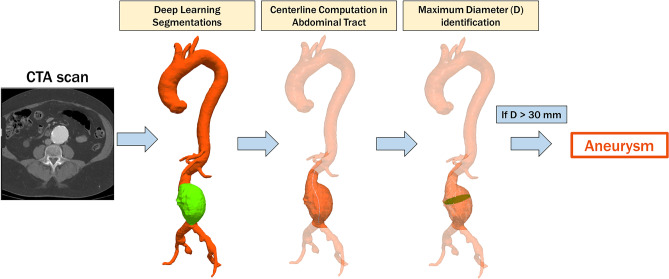
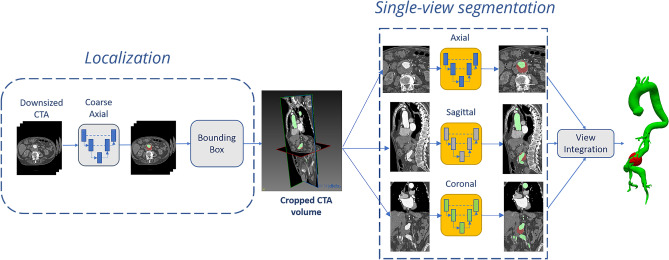
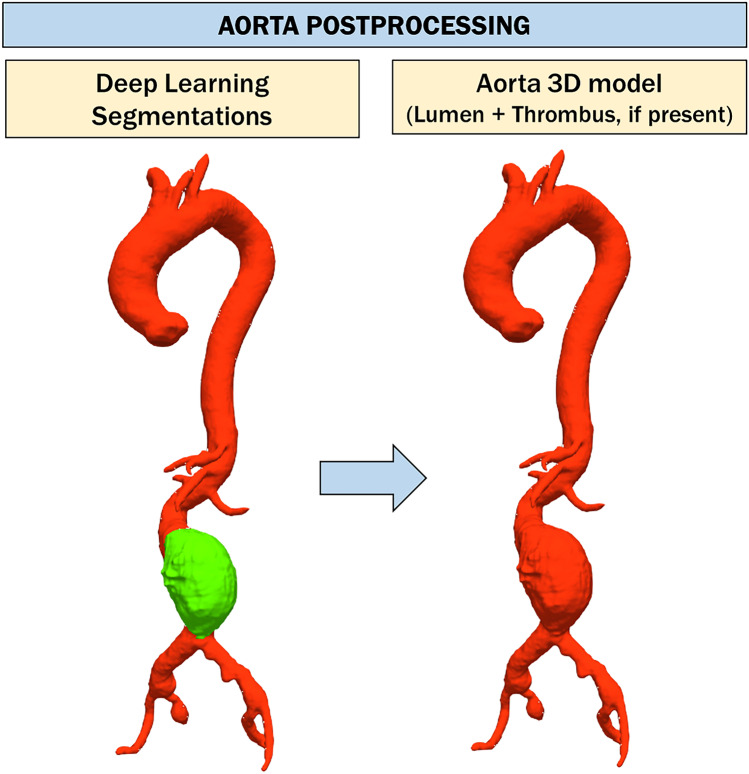
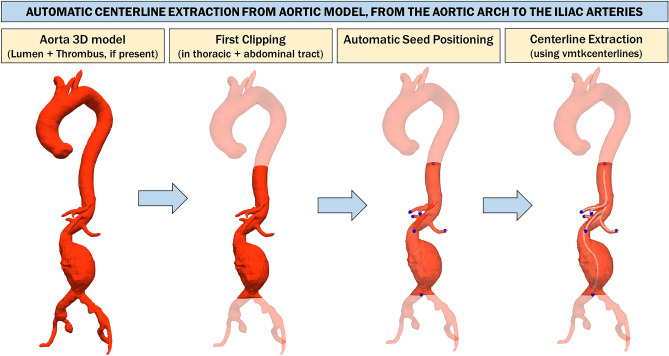
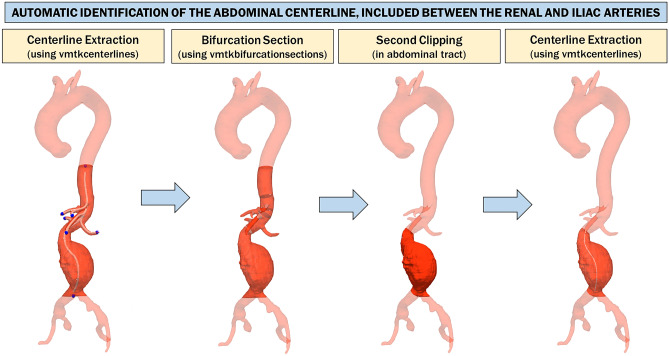
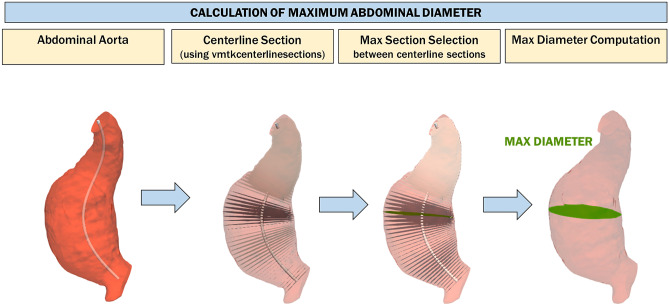
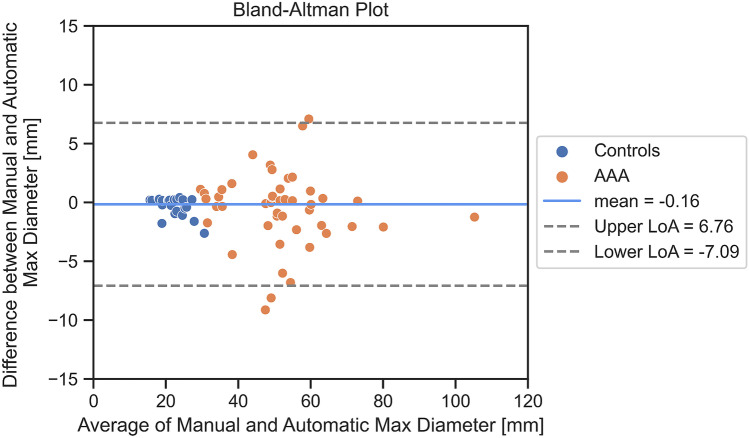
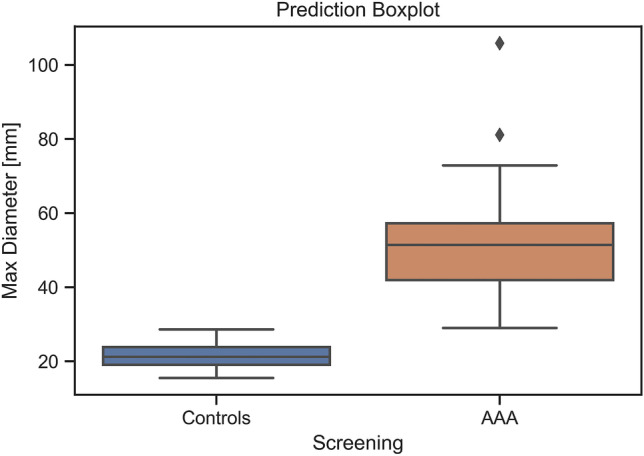
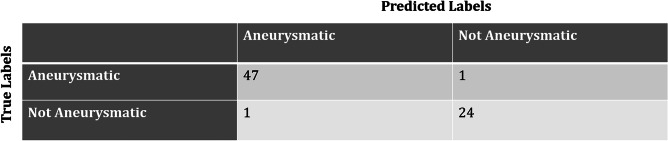
The aim of our study is to validate a totally automated deep learning (DL)-based segmentation pipeline to screen abdominal aortic aneurysms (AAA) in computed tomography angiography (CTA) scans. We retrospectively evaluated 73 thoraco-abdominal CTAs (48 AAA and 25 control CTA) by means of a DL-based segmentation pipeline built on a 2.5D convolutional neural network (CNN) architecture to segment lumen and thrombus of the aorta. The maximum aortic diameter of the abdominal tract was compared using a threshold value (30 mm). Blinded manual measurements from a radiologist were done in order to create a true comparison. The screening pipeline was tested on 48 patients with aneurysm and 25 without aneurysm. The average diameter manually measured was 51.1 ± 14.4 mm for patients with aneurysms and 21.7 ± 3.6 mm for patients without aneurysms. The pipeline correctly classified 47 AAA out of 48 and 24 control patients out of 25 with 97% accuracy, 98% sensitivity, and 96% specificity. The automated pipeline of aneurysm measurements in the abdominal tract reported a median error with regard to the maximum abdominal diameter measurement of 1.3 mm. Our approach allowed for the maximum diameter of 51.2 ± 14.3 mm in patients with aneurysm and 22.0 ± 4.0 mm in patients without an aneurysm. The DL-based screening for AAA is a feasible and accurate method, calling for further validation using a larger pool of diagnostic images towards its clinical use.
Keywords: Abdominal aortic aneurysm (AAA); Artificial intelligence (AI); Deep learning (DL); Screening.
© 2023. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures
References
-
- Wanhainen A, Verzini F, Van Herzeele I, Allaire E, Bown M, Cohnert T, Dick F, van Herwaarden J, Karkos C, Koelemay M, Kölbel T, Loftus I, Mani K, Melissano G, Powell J, Szeberin Z. Esvs Guidelines Committee, de Borst GJ, Chakfe N, Debus S, Verhagen H: Editor's Choice - European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. European journal of vascular and endovascular surgery: the official journal of the European Society for Vascular Surgery. 2019;57(1):8–93. doi: 10.1016/j.ejvs.2018.09.020. - DOI - PubMed
-
- Chaikof EL, Dalman RL, Eskandari MK, Jackson BM, Lee WA, Mansour MA, Mastracci TM, Mell M, Murad MH, Nguyen LL, Oderich GS, Patel MS, Schermerhorn ML, Starnes BW: The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. Journal of vascular surgery, 67(1), 2–77.e2, 2018.Cosford, PA, Leng GC: Screening for abdominal aortic aneurysm. The Cochrane Database of Systematic Reviews, (2), CD002945, 2007 - PubMed
-
- O’Leary SA, Kavanagh EG, Grace PA, McGloughlin TM, Doyle BJ. The biaxial mechanical behavior of abdominal aortic aneurysm intraluminal thrombus: classification of morphology and the determination of layer and region specific properties. J Biomech. 2014;47(6):1430–1437. doi: 10.1016/j.jbiomech.2014.01.041. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
