

Different definitions of feeding intolerance and their associations with outcomes of critically ill adults receiving enteral nutrition: a systematic review and meta-analysis
- PMID: 37408020
- PMCID: PMC10320932
- DOI: 10.1186/s40560-023-00674-3
Different definitions of feeding intolerance and their associations with outcomes of critically ill adults receiving enteral nutrition: a systematic review and meta-analysis
Abstract
Background: A unified clinical definition of feeding intolerance (FI) is urged for better management of enteral nutrition (EN) in critically ill patients. We aimed to identify optimum clinical FI definitions based on reported evidence.
Methods: We searched clinical studies comparing FI with non-FI with a clear definition, summarized the evidence by random-effect meta-analyses, and rated the certainty of evidence by the Grading of Recommendations Assessment, Development and Evaluation frameworks.
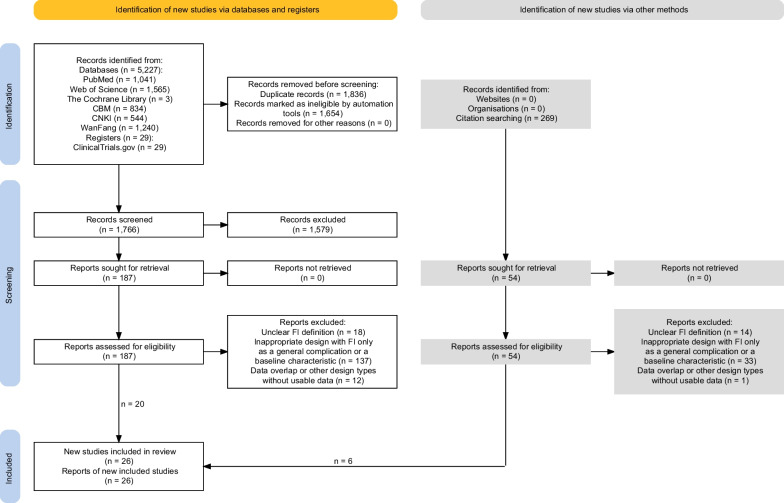
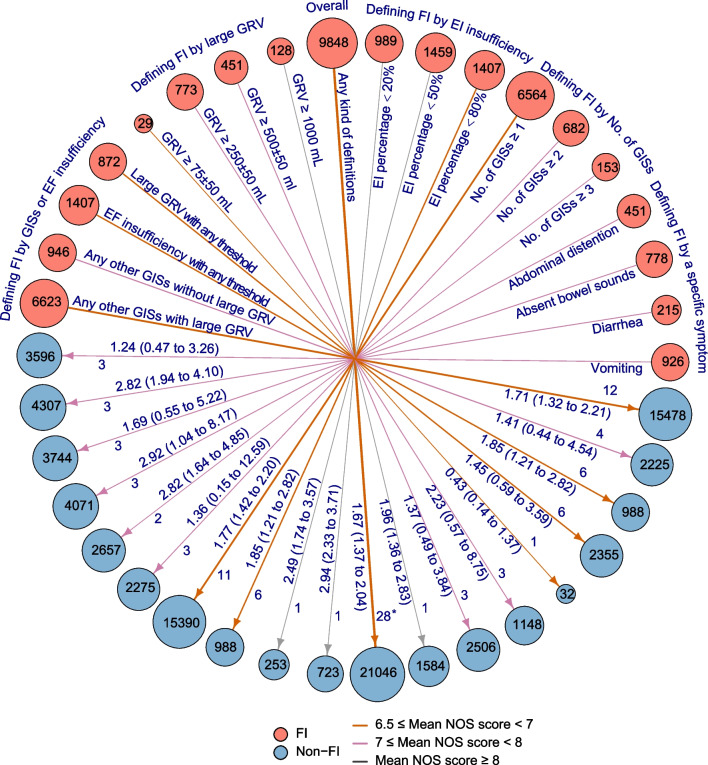
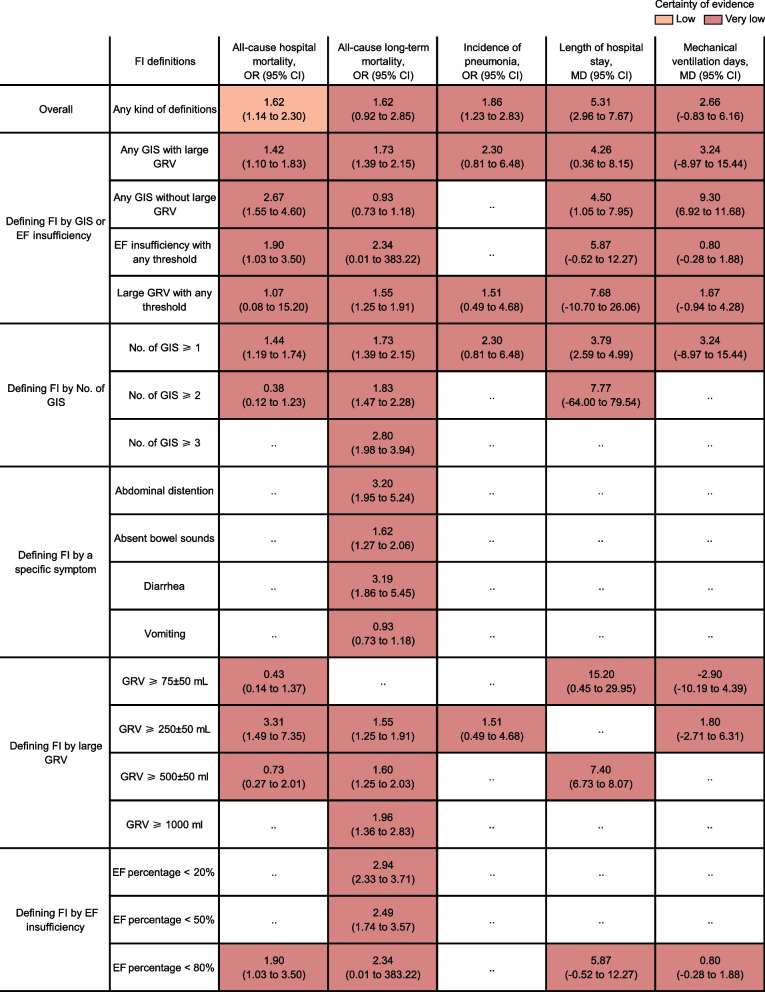
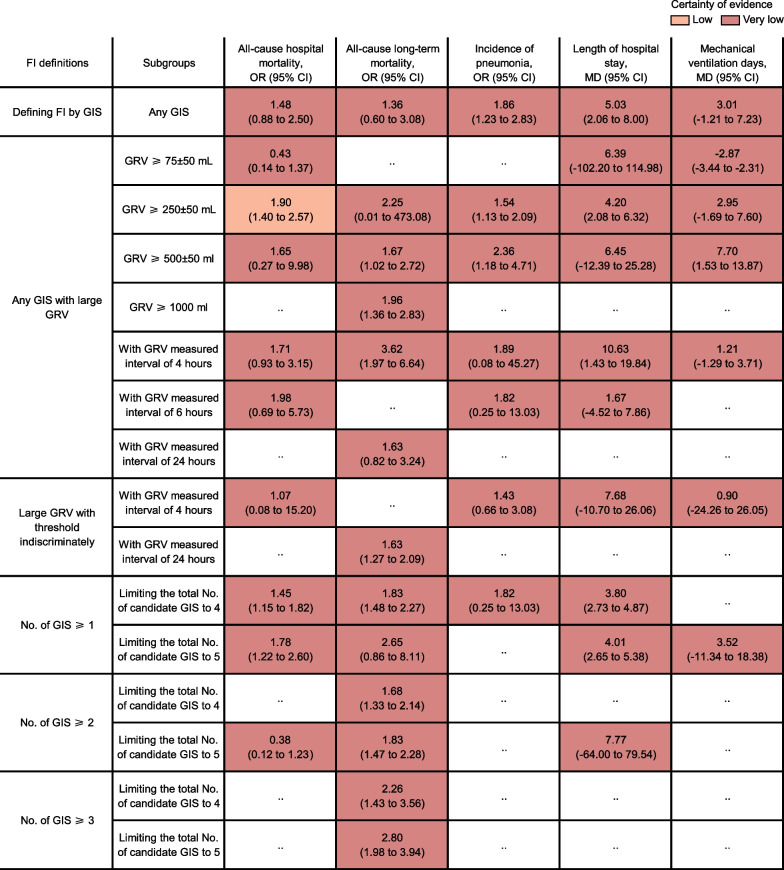
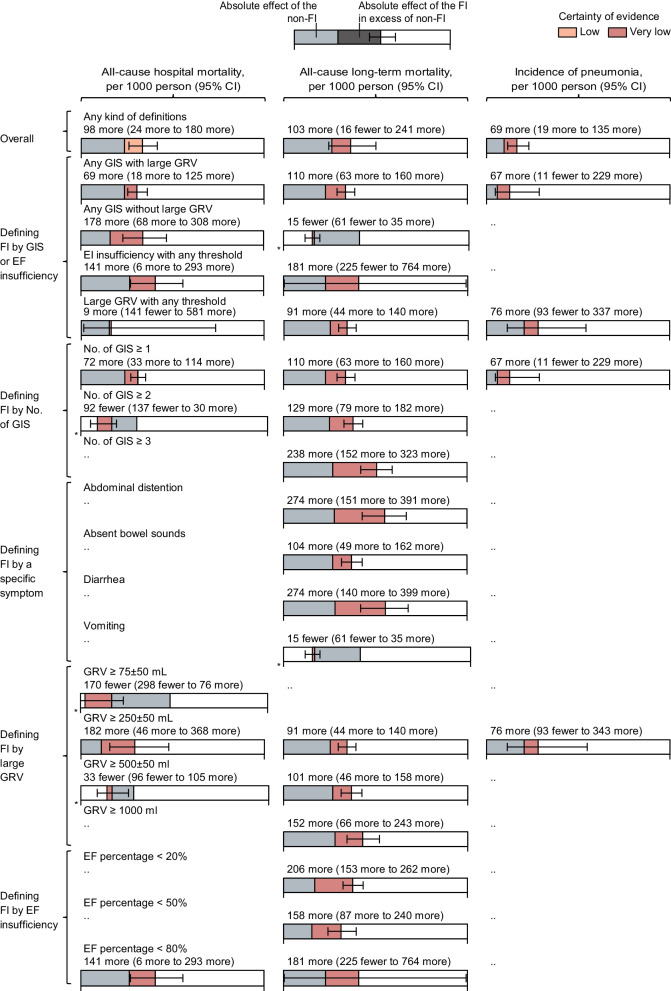
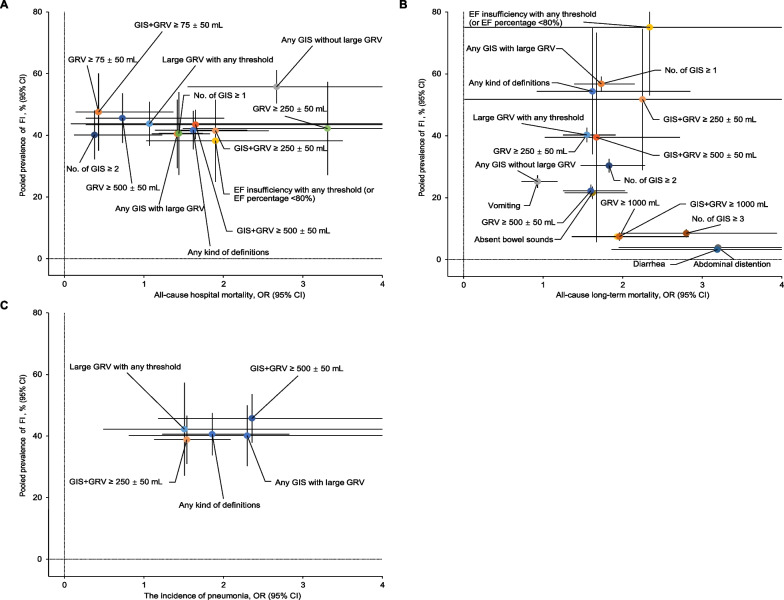
Results: Five thousand five hundred twenty-five records were identified, of which 26 eligible studies enrolled 25,189 adult patients. Most patient-centered outcomes were associated with FI overall. Low to very low certainty evidence established FI defined as large gastric residual volume (GRV) ≥ 250 ± 50 mL combined with any other gastrointestinal symptoms (GIS) had a significant association with high mortalities in particular all-cause hospital mortality (odds ratio [OR] 1.90, 95% confidence interval [CI] 1.40-2.57), the incidence of pneumonia (OR 1.54, 95% CI 1.13-2.09) and prolonged length of hospital stay (mean difference 4.20, 95% CI 2.08-6.32), with a moderate hospital prevalence (41.49%, 95% CI 31.61-51.38%). 3-day enteral feeding (EF) delivered percentage < 80% had a moderate hospital prevalence (38.23%, 95% CI 24.88-51.58) but a marginally significant association with all-cause hospital mortality (OR 1.90, 95% CI 1.03-3.50).
Conclusions: In critically ill adult patients receiving EN, the large-GRV-centered GIS to define FI seemed to be superior to 3-day EF-insufficiency in terms of both close associations with all-cause hospital mortality and acceptable hospital prevalence (Registered PROSPERO: CRD42022326273).
Trial registration: The protocol for this review and meta-analysis was registered with PROSPERO: CRD42022326273. Registered 10 May 2022.
Keywords: Critically ill adults; Definitions; Enteral nutrition; Feeding intolerance.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Reintam Blaser A, Malbrain ML, Starkopf J, Fruhwald S, Jakob SM, De Waele J, et al. Gastrointestinal function in intensive care patients: terminology, definitions and management. Recommendations of the ESICM Working Group on Abdominal Problems. Intensive Care Med. 2012;38:384–394. doi: 10.1007/s00134-011-2459-y. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
