

Comparisons of perioperative and long-term outcomes of laparoscopic versus open gastrectomy for advanced gastric cancer after neoadjuvant therapy: an updated pooled analysis of eighteen studies
- PMID: 37408041
- PMCID: PMC10320971
- DOI: 10.1186/s40001-023-01197-1
Comparisons of perioperative and long-term outcomes of laparoscopic versus open gastrectomy for advanced gastric cancer after neoadjuvant therapy: an updated pooled analysis of eighteen studies
Abstract
Background: Outcomes of laparoscopic surgery in advanced gastric cancer patients who received neoadjuvant therapy represent a controversial issue. We performed an updated meta-analysis to evaluate the perioperative and long-term survival outcomes of laparoscopic gastrectomy (LG) versus conventional open gastrectomy (OG) in this subset of patients.
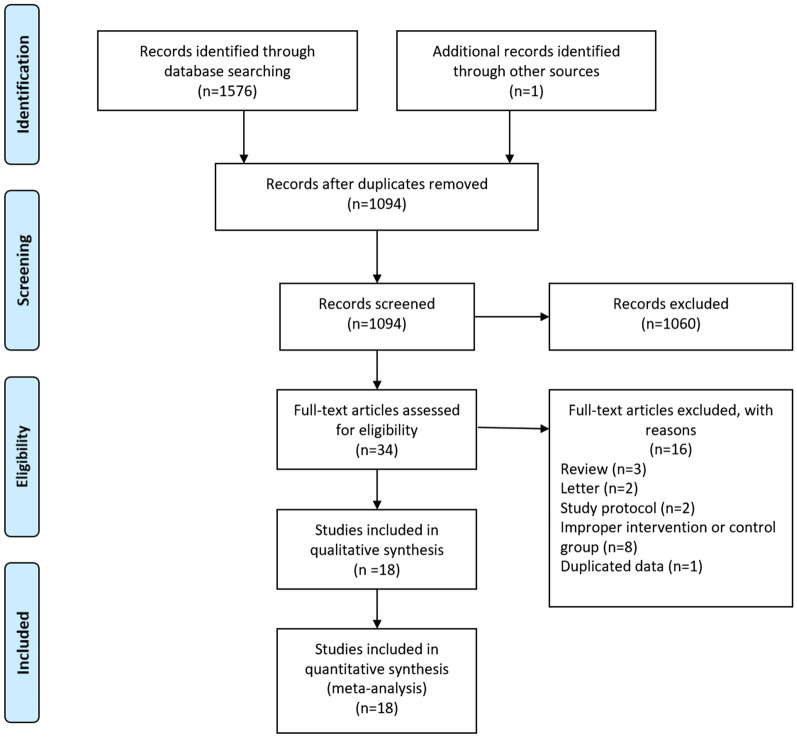
Methods: Electronic databases including PubMed, Embase, Web of Science, the Cochrane Central Register of Controlled Trials and China National Knowledge Infrastructure were comprehensively searched up to May 2023. The short-term and long-term outcomes of LG versus OG in advanced gastric cancer patients undergoing neoadjuvant therapy were evaluated. Effect sizes with 95% confidence intervals were always assessed using random-effects model. The prospective protocol was registered with PROSPERO (CRD42022359126).
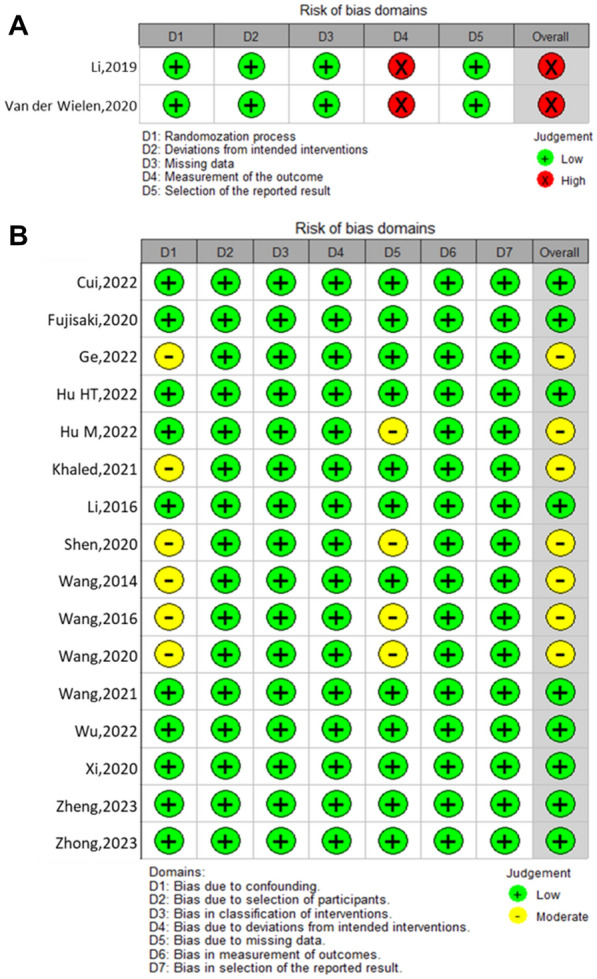
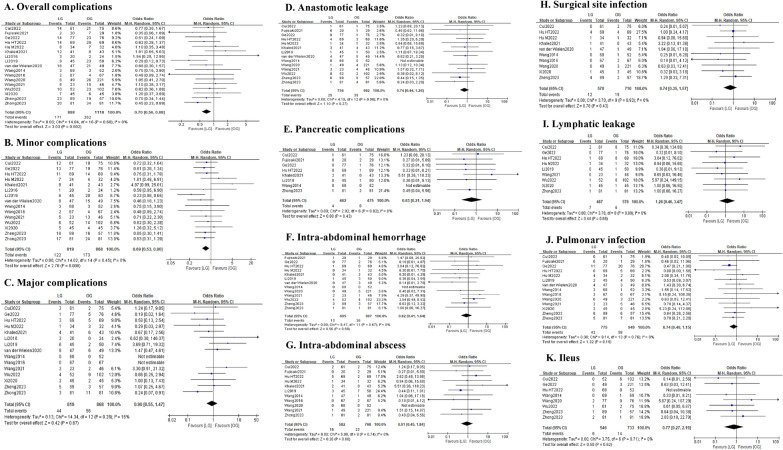
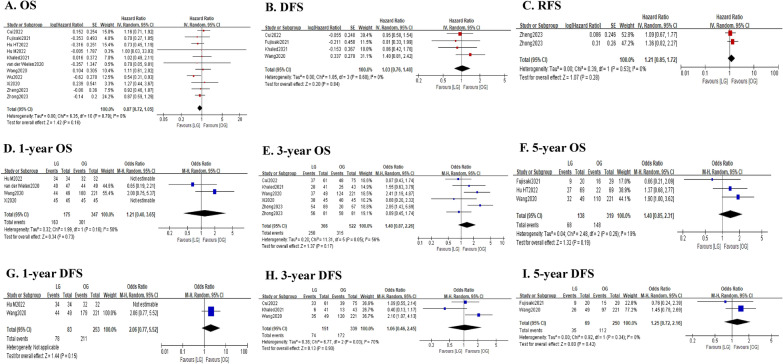
Results: Eighteen studies (2 randomized controlled trials and 16 cohort studies) involving 2096 patients were included. In total, 933 patients were treated with LG and 1163 patients were treated with OG. In perioperative outcomes, LG was associated with less estimated blood loss (MD = - 65.15; P < 0.0001), faster time to flatus (MD = - 0.56; P < 0.0001) and liquid intake (MD = - 0.42; P = 0.02), reduced hospital stay (MD = - 2.26; P < 0.0001), lower overall complication rate (OR = 0.70; P = 0.002) and lower minor complication rate (OR = 0.69; P = 0.006), while longer operative time (MD = 25.98; P < 0.0001). There were no significant differences between the two groups in terms of proximal margin, distal margin, R1/R2 resection rate, retrieved lymph nodes, time to remove gastric tube and drainage tube, major complications and other specific complications. In survival outcomes, LG and OG were not significantly different in overall survival, disease-free survival and recurrence-free survival.
Conclusion: LG can be a safe and feasible technique for the treatment of advanced gastric cancer patients receiving neoadjuvant therapy. However, more high-quality randomized controlled trials are still needed to further validate the results of our study.
Keywords: Gastric cancer; Laparoscopic gastrectomy; Meta-analysis; Neoadjuvant therapy; Open gastrectomy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
