

The impact of pharmacist interventions, follow-up frequency and default on glycemic control in Diabetes Medication Therapy Adherence Clinic program: a multicenter study in Malaysia
- PMID: 37408067
- PMCID: PMC10320936
- DOI: 10.1186/s40545-023-00583-8
The impact of pharmacist interventions, follow-up frequency and default on glycemic control in Diabetes Medication Therapy Adherence Clinic program: a multicenter study in Malaysia
Abstract
Background: Pharmacist's involvement in optimizing medication adherence among diabetic patients has been implemented for over a decade. Diabetes Medication Therapy Adherence Clinic (DMTAC) was set up to educate diabetic patients, monitor treatment outcomes, and manage drug-related problems. While evidence shows that pharmacist-led DMTAC was effective in reducing HbA1c, there was limited data regarding the impact of different intervention types and default to follow-up on glycemic control.
Aim: To assess the impact DMTAC on glycemic control and the difference in glycemic control between hospital and health clinic settings as well as defaulter and non-defaulter. In addition, the impact of pharmacist's interventions, DMTAC follow-up frequencies, and duration of diabetes on glycemic control were also determined.
Methods: A retrospective study was conducted among diabetes patients under DMTAC care between January 2019 and June 2020 in five hospitals and 23 primary health clinics. Patients' demographics data, treatment regimens, frequencies of DMTAC visits, defaulter (absent from DMTAC visits) and types of pharmacists' intervention were retrieved from patients' medical records and electronic database. HbA1c was collected at baseline, 4-6 months (post-1), and 8-12 months (post-2).
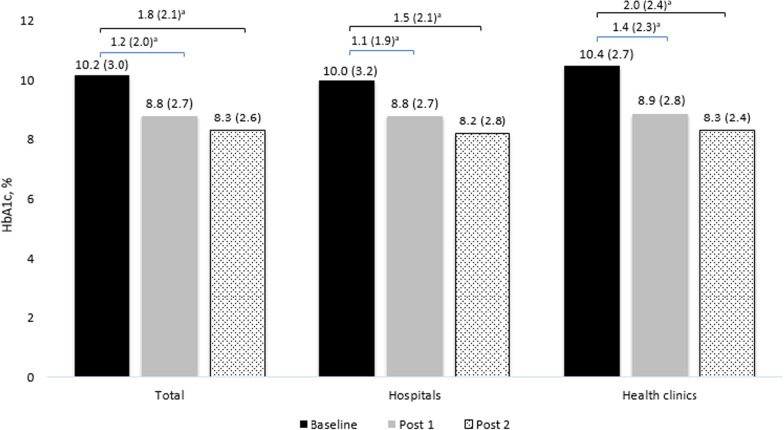
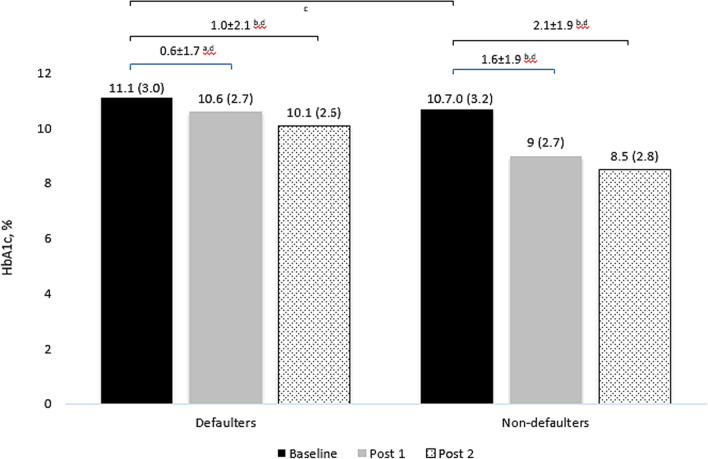
Results: We included 956 patients, of which 60% were females with a median age of 58.0 (IQR: 5.0) years. Overall, the HbA1c reduced significantly from baseline (median: 10.2, IQR: 3.0) to post-1 (median: 8.8, IQR: 2.7) and post-2 (median: 8.3, IQR: 2.6%) (p < 0.001). There were 4317 pharmacists' interventions performed, with the majority being dosage adjustment (n = 2407, 55.8%), followed by lab investigations (849, 19.7%), drugs addition (653, 15.1%), drugs discontinuation (408, 9.5%). Patients treated in hospitals received significantly more interventions than those treated in primary health clinics (p < 0.001). We observed significantly less reduction in HbA1c in DMTAC follow-up defaulters than non-defaulters after 1 year (- 1.02% vs. - 2.14%, p = 0.001). Frequencies of DMTAC visits (b: 0.19, CI: 0.079-0.302, p = 0.001), number of dosage adjustments (b: 0.83, CI: 0.015-0.151, p = 0.018) and number of additional drugs recommended (b: 0.37, CI: 0.049-0.691, p = 0.024) had positive impact on glycemic control whereas duration of diabetes (b: - 0.0302, CI: - 0.0507, - 0.007, p = 0.011) had negative impact.
Conclusion: Glycemic control improved significantly and sustained up to one year among patients in pharmacists-led DMTAC. However, DMTAC defaulters experienced poorer glycemic control. Considering more frequent visits and targeted interventions by pharmacists at DMTAC resulted in improved HbA1c control, these strategies should be taken into account for future program planning.
Keywords: Default; Diabetes; Glycemic control; HbA1c; Interventions; Malaysia; Pharmacists; Visits.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Evaluation of a pharmacist-managed diabetes medication therapy adherence clinic.Pharm Pract (Granada). 2010 Oct;8(4):250-4. doi: 10.4321/s1886-36552010000400008. Epub 2010 Mar 15. Pharm Pract (Granada). 2010. PMID: 25126149 Free PMC article.
-
The effectiveness of diabetes medication therapy adherence clinic to improve glycaemic control among patients with type 2 diabetes mellitus: a randomised controlled trial.Med J Malaysia. 2020 May;75(3):246-253. Med J Malaysia. 2020. PMID: 32467540 Clinical Trial.
-
The influence of pharmacist-led collaborative care on clinical outcomes in type 2 diabetes mellitus: a multicenter randomized control trial.Front Public Health. 2024 Feb 27;12:1323102. doi: 10.3389/fpubh.2024.1323102. eCollection 2024. Front Public Health. 2024. PMID: 38476498 Free PMC article. Clinical Trial.
-
The Pharmacist's role in dermatology: Patient medication adherence.J Dermatol. 2023 Sep;50(9):1099-1107. doi: 10.1111/1346-8138.16895. Epub 2023 Jul 25. J Dermatol. 2023. PMID: 37489577 Review.
-
The impact of pharmacist care on diabetes outcomes in primary care settings: An umbrella review of published systematic reviews.Prim Care Diabetes. 2020 Oct;14(5):393-400. doi: 10.1016/j.pcd.2019.12.007. Epub 2020 Jan 8. Prim Care Diabetes. 2020. PMID: 31926868
Cited by
-
Impact of Attendance to a Pharmacist-Managed Medication Adherence Clinic on Glycemic Control and Risk Factors for Non-Completion Among Persons with Type 2 Diabetes Mellitus in Selangor, Malaysia.Ther Clin Risk Manag. 2024 Aug 12;20:495-503. doi: 10.2147/TCRM.S442026. eCollection 2024. Ther Clin Risk Manag. 2024. PMID: 39156759 Free PMC article.
-
Development and validation of patient diabetes knowledge questionnaire (PDKQ).J Pharm Policy Pract. 2023 Oct 19;16(1):121. doi: 10.1186/s40545-023-00631-3. J Pharm Policy Pract. 2023. PMID: 37858279 Free PMC article.
-
Association between follow-up visit frequency, medication types prescribed, and glycaemic outcomes among diabetic patients in China's Basic Public Health Services programme: a retrospective cohort study.BMJ Public Health. 2025 Jul 22;3(2):e001245. doi: 10.1136/bmjph-2024-001245. eCollection 2025. BMJ Public Health. 2025. PMID: 40734964 Free PMC article.
References
-
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Lond Engl. 2016;388:1659–724. - PMC - PubMed
-
- International Diabetes Federation. International Diabetes Federation Diabetes Atlas.
-
- National Health and Morbidity Survey. Institute for Public Health, Ministry of Health Malaysia; 2019.
LinkOut - more resources
Full Text Sources
Miscellaneous