

Extended prone positioning for intubated ARDS: a review
- PMID: 37408074
- PMCID: PMC10320968
- DOI: 10.1186/s13054-023-04526-2
Extended prone positioning for intubated ARDS: a review
Abstract
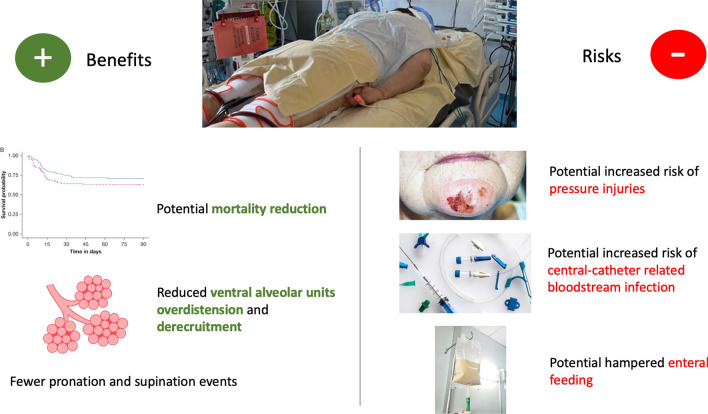
During the COVID-19 pandemic, several centers had independently reported extending prone positioning beyond 24 h. Most of these centers reported maintaining patients in prone position until significant clinical improvement was achieved. One center reported extending prone positioning for organizational reasons relying on a predetermined fixed duration. A recent study argued that a clinically driven extension of prone positioning beyond 24 h could be associated with reduced mortality. On a patient level, the main benefit of extending prone positioning beyond 24 h is to maintain a more homogenous distribution of the gas-tissue ratio, thus delaying the increase in overdistention observed when patients are returned to the supine position. On an organizational level, extending prone positioning reduces the workload for both doctors and nurses, which might significantly enhance the quality of care in an epidemic. It might also reduce the incidence of accidental catheter and tracheal tube removal, thereby convincing intensive care units with low incidence of ARDS to prone patients more systematically. The main risk associated with extended prone positioning is an increased incidence of pressure injuries. Up until now, retrospective studies are reassuring, but prospective evaluation is needed.
Keywords: Acute respiratory distress syndrome; Extended prone positioning; Mechanical ventilation; Prolonged prone positioning; Prone positioning.
© 2023. The Author(s).
Conflict of interest statement
Jean-Damien Ricard: Fisher&Paykel covered travel expenses and provide high flow devices to a multicenter randomized control trial which JD Ricard is working on the use of nasal high flow in patients with acute hypercapnic respiratory failure. Thaïs Walter declares she has no competing interests.
Figures
Similar articles
-
Extended prone positioning duration for COVID-19-related ARDS: benefits and detriments.Crit Care. 2022 Jul 8;26(1):208. doi: 10.1186/s13054-022-04081-2. Crit Care. 2022. PMID: 35804453 Free PMC article.
-
The impact of patient positioning on pressure ulcers in patients with severe ARDS: results from a multicentre randomised controlled trial on prone positioning.Intensive Care Med. 2014 Mar;40(3):397-403. doi: 10.1007/s00134-013-3188-1. Epub 2013 Dec 19. Intensive Care Med. 2014. PMID: 24352484 Clinical Trial.
-
The efficacy and tolerance of prone positioning in non-intubation patients with acute hypoxemic respiratory failure and ARDS: a meta-analysis.Ther Adv Respir Dis. 2021 Jan-Dec;15:17534666211009407. doi: 10.1177/17534666211009407. Ther Adv Respir Dis. 2021. PMID: 33888007 Free PMC article.
-
Prone positioning for ARDS patients-tips for preparation and use during the COVID-19 pandemic.Can J Anaesth. 2021 Apr;68(4):541-545. doi: 10.1007/s12630-020-01885-0. Epub 2020 Dec 24. Can J Anaesth. 2021. PMID: 33367994 Free PMC article. Review.
-
Effect of prone positioning on oxygenation and static respiratory system compliance in COVID-19 ARDS vs. non-COVID ARDS.Respir Res. 2021 Aug 6;22(1):220. doi: 10.1186/s12931-021-01819-4. Respir Res. 2021. PMID: 34362368 Free PMC article. Review.
Cited by
-
Extended Prone Position and 90-Day Mortality in Mechanically Ventilated Patients With COVID-19.Respir Care. 2024 Sep 26;69(10):1255-1265. doi: 10.4187/respcare.11622. Respir Care. 2024. PMID: 39137953
-
Improving oxygenation in a patient with respiratory failure due to morbid obesity by applying airway pressure release ventilation: a case report.J Med Case Rep. 2024 Aug 5;18(1):353. doi: 10.1186/s13256-024-04665-2. J Med Case Rep. 2024. PMID: 39098947 Free PMC article.
-
The effects of prolonged prone positioning on response and prognosis in patients with acute respiratory distress syndrome: a retrospective cohort study.J Intensive Care. 2025 May 7;13(1):24. doi: 10.1186/s40560-025-00795-x. J Intensive Care. 2025. PMID: 40336057 Free PMC article.
-
Respiratory effects of prone position in COVID-19 acute respiratory distress syndrome differ according to the recruitment-to-inflation ratio: a prospective observational study.Ann Intensive Care. 2024 Sep 18;14(1):146. doi: 10.1186/s13613-024-01375-2. Ann Intensive Care. 2024. PMID: 39292429 Free PMC article.
-
Recruitment-Potential-Oriented Mechanical Ventilation Protocol and Narrative Review for Patients with Acute Respiratory Distress Syndrome.J Pers Med. 2024 Jul 23;14(8):779. doi: 10.3390/jpm14080779. J Pers Med. 2024. PMID: 39201971 Free PMC article.
References
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An official American thoracic society/European society of intensive care medicine/society of critical care medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–1263. doi: 10.1164/rccm.201703-0548ST. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
