

Immunomodulatory Macrophages Enable E-MNC Therapy for Radiation-Induced Salivary Gland Hypofunction
- PMID: 37408251
- PMCID: PMC10216929
- DOI: 10.3390/cells12101417
Immunomodulatory Macrophages Enable E-MNC Therapy for Radiation-Induced Salivary Gland Hypofunction
Abstract
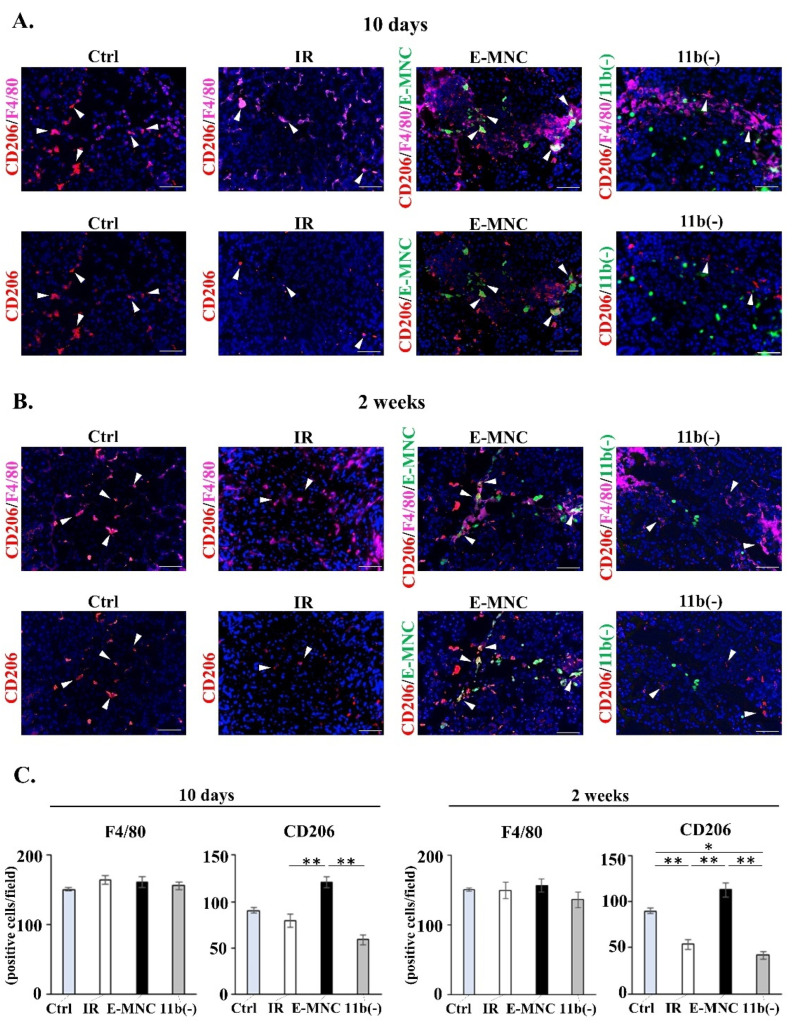
A newly developed therapy using effective-mononuclear cells (E-MNCs) is reportedly effective against radiation-damaged salivary glands (SGs) due to anti-inflammatory and revascularization effects. However, the cellular working mechanism of E-MNC therapy in SGs remains to be elucidated. In this study, E-MNCs were induced from peripheral blood mononuclear cells (PBMNCs) by culture for 5-7 days in medium supplemented with five specific recombinant proteins (5G-culture). We analyzed the anti-inflammatory characteristics of macrophage fraction of E-MNCs using a co-culture model with CD3/CD28-stimulated PBMNCs. To test therapeutic efficacy in vivo, either E-MNCs or E-MNCs depleted of CD11b-positive cells were transplanted intraglandularly into mice with radiation-damaged SGs. Following transplantation, SG function recovery and immunohistochemical analyses of harvested SGs were assessed to determine if CD11b-positive macrophages contributed to tissue regeneration. The results indicated that CD11b/CD206-positive (M2-like) macrophages were specifically induced in E-MNCs during 5G-culture, and Msr1- and galectin3-positive cells (immunomodulatory macrophages) were predominant. CD11b-positive fraction of E-MNCs significantly inhibited the expression of inflammation-related genes in CD3/CD28-stimulated PBMNCs. Transplanted E-MNCs exhibited a therapeutic effect on saliva secretion and reduced tissue fibrosis in radiation-damaged SGs, whereas E-MNCs depleted of CD11b-positive cells and radiated controls did not. Immunohistochemical analyses revealed HMGB1 phagocytosis and IGF1 secretion by CD11b/Msr1-positive macrophages from both transplanted E-MNCs and host M2-macrophages. Thus, the anti-inflammatory and tissue-regenerative effects observed in E-MNC therapy against radiation-damaged SGs can be partly explained by the immunomodulatory effect of M2-dominant macrophage fraction.
Keywords: cell therapy; macrophage; peripheral blood mononuclear cells; radiation-induced damage; salivary gland.
Conflict of interest statement
The authors declare no competing financial interests or personal relationships that could influence this research.
Figures











References
-
- Vissink A., Burlage F.R., Spijkervet F.K.L., Jansma J., Coppes R.P. Prevention and treatment of the consequences of head and neck radiotherapy: A Critical Review. Oral. Biol. Med. 2003;14:213–225. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
