

Prediction of posttraumatic functional recovery in middle-aged and older patients through dynamic ensemble selection modeling
- PMID: 37408743
- PMCID: PMC10319009
- DOI: 10.3389/fpubh.2023.1164820
Prediction of posttraumatic functional recovery in middle-aged and older patients through dynamic ensemble selection modeling
Abstract
Introduction: Age-specific risk factors may delay posttraumatic functional recovery; complex interactions exist between these factors. In this study, we investigated the prediction ability of machine learning models for posttraumatic (6 months) functional recovery in middle-aged and older patients on the basis of their preexisting health conditions.
Methods: Data obtained from injured patients aged ≥45 years were divided into training-validation (n = 368) and test (n = 159) data sets. The input features were the sociodemographic characteristics and baseline health conditions of the patients. The output feature was functional status 6 months after injury; this was assessed using the Barthel Index (BI). On the basis of their BI scores, the patients were categorized into functionally independent (BI >60) and functionally dependent (BI ≤60) groups. The permutation feature importance method was used for feature selection. Six algorithms were validated through cross-validation with hyperparameter optimization. The algorithms exhibiting satisfactory performance were subjected to bagging to construct stacking, voting, and dynamic ensemble selection models. The best model was evaluated on the test data set. Partial dependence (PD) and individual conditional expectation (ICE) plots were created.
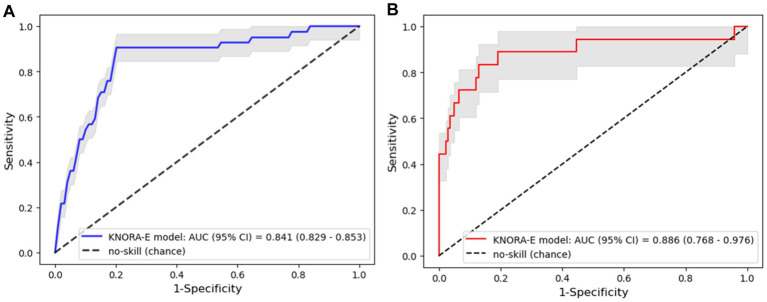
Results: In total, nineteen of twenty-seven features were selected. Logistic regression, linear discrimination analysis, and Gaussian Naive Bayes algorithms exhibited satisfactory performances and were, therefore, used to construct ensemble models. The k-Nearest Oracle Elimination model outperformed the other models when evaluated on the training-validation data set (sensitivity: 0.732, 95% CI: 0.702-0.761; specificity: 0.813, 95% CI: 0.805-0.822); it exhibited compatible performance on the test data set (sensitivity: 0.779, 95% CI: 0.559-0.950; specificity: 0.859, 95% CI: 0.799-0.912). The PD and ICE plots showed consistent patterns with practical tendencies.
Conclusion: Preexisting health conditions can predict long-term functional outcomes in injured middle-aged and older patients, thus predicting prognosis and facilitating clinical decision-making.
Keywords: dynamic ensemble selection; machine learning; middle-aged patient; older patient; traumatic injury.
Copyright © 2023 Nhu, Kang, Yeh, Wu, Tsai, Piravej and Lam.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Low LL, Kwan YH, Ko MSM, Yeam CT, Lee VSY, Tan WB, et al. Epidemiologic characteristics of multimorbidity and sociodemographic factors associated with multimorbidity in a rapidly aging Asian country. JAMA Netw Open. (2019) 2:e1915245. doi: 10.1001/jamanetworkopen.2019.15245, PMID: - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources