

Artificial intelligence-driven prediction of COVID-19-related hospitalization and death: a systematic review
- PMID: 37408750
- PMCID: PMC10319067
- DOI: 10.3389/fpubh.2023.1183725
Artificial intelligence-driven prediction of COVID-19-related hospitalization and death: a systematic review
Abstract
Aim: To perform a systematic review on the use of Artificial Intelligence (AI) techniques for predicting COVID-19 hospitalization and mortality using primary and secondary data sources.
Study eligibility criteria: Cohort, clinical trials, meta-analyses, and observational studies investigating COVID-19 hospitalization or mortality using artificial intelligence techniques were eligible. Articles without a full text available in the English language were excluded.
Data sources: Articles recorded in Ovid MEDLINE from 01/01/2019 to 22/08/2022 were screened.
Data extraction: We extracted information on data sources, AI models, and epidemiological aspects of retrieved studies.
Bias assessment: A bias assessment of AI models was done using PROBAST.
Participants: Patients tested positive for COVID-19.
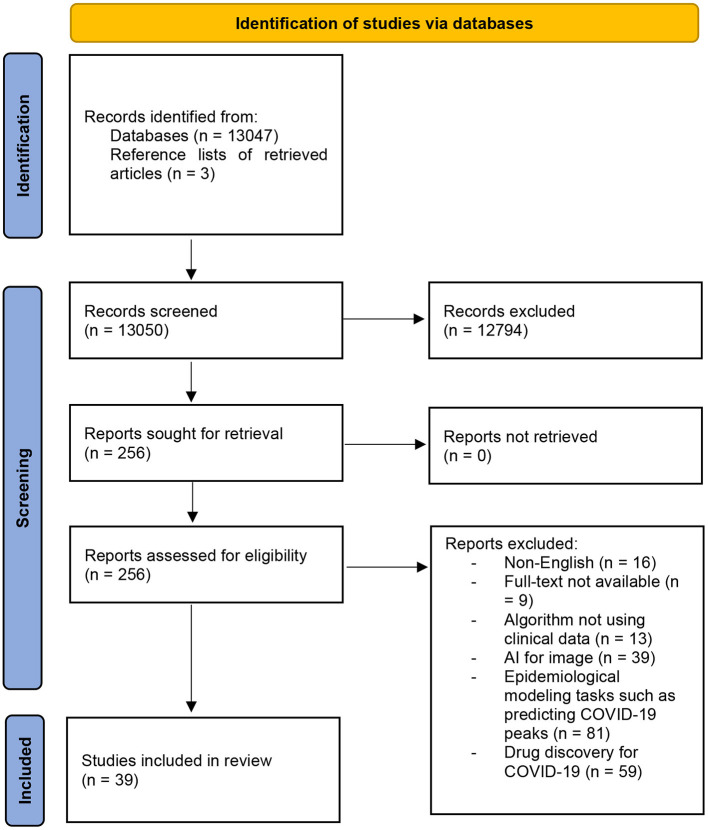
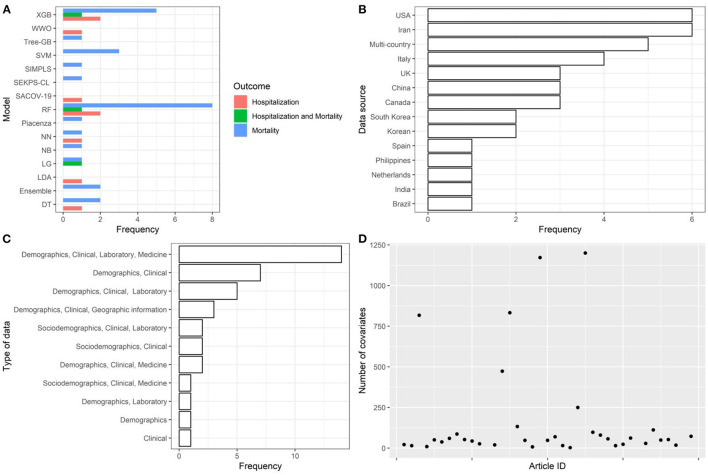
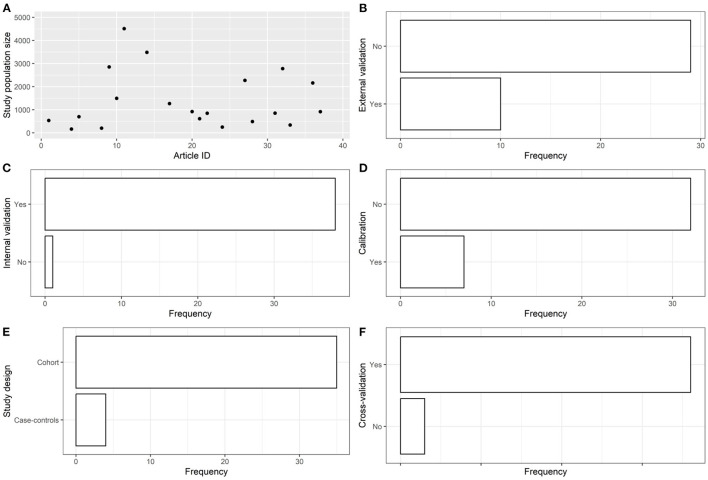
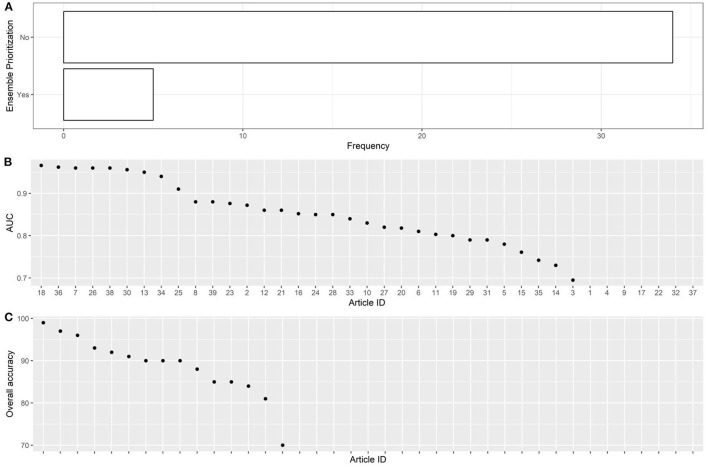
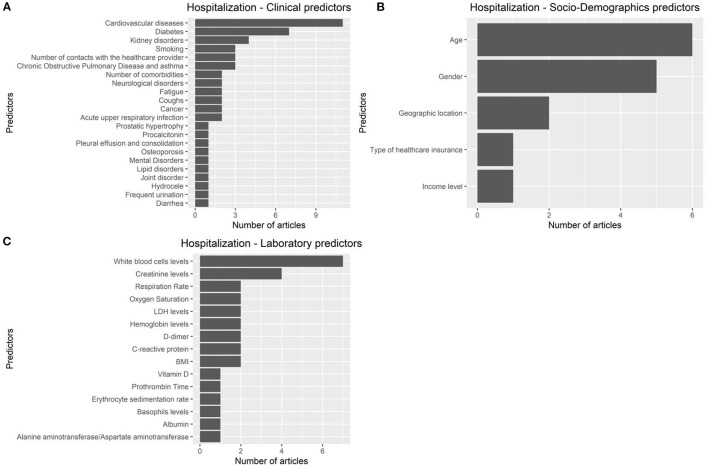
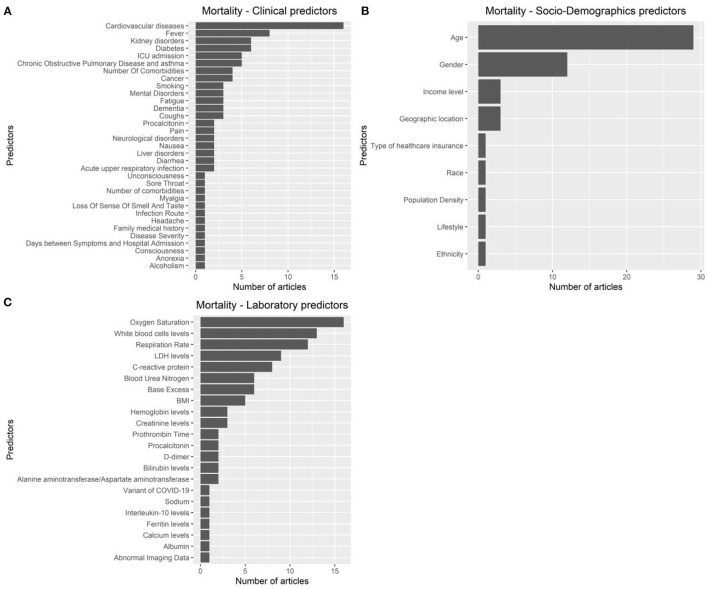
Results: We included 39 studies related to AI-based prediction of hospitalization and death related to COVID-19. The articles were published in the period 2019-2022, and mostly used Random Forest as the model with the best performance. AI models were trained using cohorts of individuals sampled from populations of European and non-European countries, mostly with cohort sample size <5,000. Data collection generally included information on demographics, clinical records, laboratory results, and pharmacological treatments (i.e., high-dimensional datasets). In most studies, the models were internally validated with cross-validation, but the majority of studies lacked external validation and calibration. Covariates were not prioritized using ensemble approaches in most of the studies, however, models still showed moderately good performances with Area under the Receiver operating characteristic Curve (AUC) values >0.7. According to the assessment with PROBAST, all models had a high risk of bias and/or concern regarding applicability.
Conclusions: A broad range of AI techniques have been used to predict COVID-19 hospitalization and mortality. The studies reported good prediction performance of AI models, however, high risk of bias and/or concern regarding applicability were detected.
Keywords: AI; COVID-19; PROBAST; bias; pharmacoepidemiology; predictive modeling.
Copyright © 2023 Shakibfar, Nyberg, Li, Zhao, Nordeng, Sandve, Pavlovic, Hajiebrahimi, Andersen and Sessa.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- WorldoMeter . COVID-19 CORONAVIRUS PANDEMIC. (2022). p. 1. Available online at: https://www.worldometers.info/coronavirus/ (accessed December 1, 2022).
-
- CDC. Update on COVID-19–Related Deaths. (2022). p. 1. Available online at: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html (accessed December 1, 2022).
-
- Ourworldindata. Number of COVID-19 Patients in Hospital Per Million. (2022). p. 1. Available online at: https://ourworldindata.org/grapher/current-covid-hospitalizations-per-mi... (accessed December 15, 2022).
-
- Dictionary OE. Artificial Intelligence. (2018). Available online at: https//www lexico com/definition/artificial_intelligence ( accessed July 7, 2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical