

Combination of multiparametric magnetic resonance imaging and transperineal template-guided mapping prostate biopsy to determine potential candidates for focal therapy
- PMID: 37409092
- PMCID: PMC10318325
- DOI: 10.1016/j.prnil.2022.12.003
Combination of multiparametric magnetic resonance imaging and transperineal template-guided mapping prostate biopsy to determine potential candidates for focal therapy
Abstract
Background: We assessed the ability of the combination of multiparametric magnetic resonance imaging (mpMRI) and transperineal template-guided mapping biopsy (TTMB) to determine the eligibility for focal therapy (FT) (hemiablation) in men and compared it with that of histology from radical prostatectomy (RP) specimens.
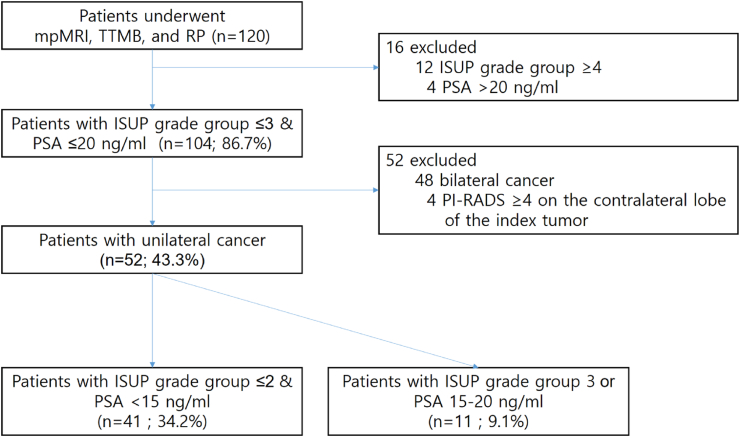
Materials and methods: In this study, 120 men who underwent mpMRI, TTMB, and RP in a single tertiary center from May 2017 to June 2021 were analyzed. The criteria of hemiablation eligibility were unilateral low-to intermediate-risk prostate cancer (limited to a maximum of International Society of Urological Pathology (ISUP) grade group 3 and prostate-specific antigen (PSA) <20 ng/mL) and clinical stage ≤T2. Evidence of non-organ-confined disease or contralateral Prostate Imaging Reporting and Data System (PI-RADS) v2 score ≥4 on mpMRI was classified as ineligible for hemiablation. Clinically significant cancer at RP was defined as any of the following: (1) ISUP grade group 1 with tumor volume ≥1.3 mL; (2) ISUP grade group ≥2; or (3) the presence of advanced stage (≥pT3).
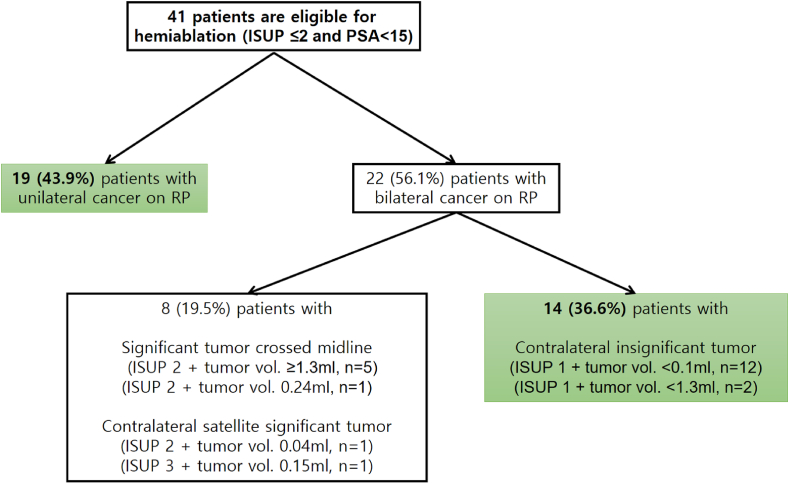
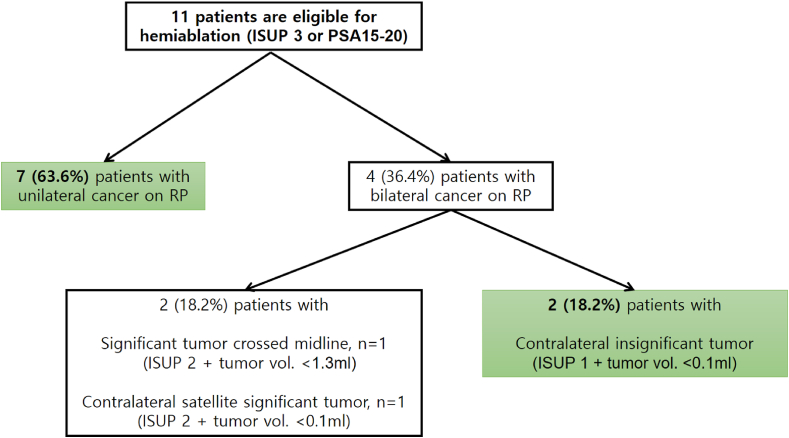
Results: Of the 120 men, data of 52 men who met the selection criteria for hemiablation were compared with final RP findings. Of these 52 men, 42 (80.7%) could be considered suitable for hemiablation on RP. The sensitivity, specificity, and accuracy of mpMRI and TTMB in predicting FT eligibility were 80.7%, 85.1%, and 82.5%, respectively. The rate of undetected contralateral significant cancer was 10 (19.2%) on mpMRI and TTMB. Six had bilateral significant cancer and four had small volumes of ISUP grade group ≥2.
Conclusions: The combination of mpMRI and TTMB substantially improves the prediction of potential candidates for hemiablation based on consensus recommendations. Improved selection criteria and further investigative tools are required to improve patient selection for hemiablation.
Keywords: Focal therapy; Hemiablation; Magnetic resonance imaging; Prostate biopsy; Prostate cancer.
© 2023 The Asian Pacific Prostate Society. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures
References
-
- Mottet N., Bellmunt J., Bolla M., Briers E., Cumberbatch M.G., De Santis M., et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2017;71(4):618–629. - PubMed
-
- Mottet N., van den Bergh R.C.N., Briers E., Van den Broeck T., Cumberbatch M.G., De Santis M., et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2021;79(2):243–262. - PubMed
-
- Wilt T.J., MacDonald R., Rutks I., Shamliyan T.A., Taylor B.C., Kane R.L. Systematic review: comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann Intern Med. 2008;148(6):435–448. - PubMed
-
- Boorjian S.A., Eastham J.A., Graefen M., Guillonneau B., Karnes R.J., Moul J.W., et al. A critical analysis of the long-term impact of radical prostatectomy on cancer control and function outcomes. Eur Urol. 2012;61(4):664–675. - PubMed
-
- Lardas M., Liew M., van den Bergh R.C., De Santis M., Bellmunt J., Van den Broeck T., et al. Quality of life outcomes after primary treatment for clinically localised prostate cancer: a systematic review. Eur Urol. 2017;72(6):869–885. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous