

Modified underwater endoscopic mucosal resection for intermediate-sized sessile colorectal polyps
- PMID: 37409275
- PMCID: PMC10318795
- DOI: 10.3389/fmed.2023.1200145
Modified underwater endoscopic mucosal resection for intermediate-sized sessile colorectal polyps
Abstract
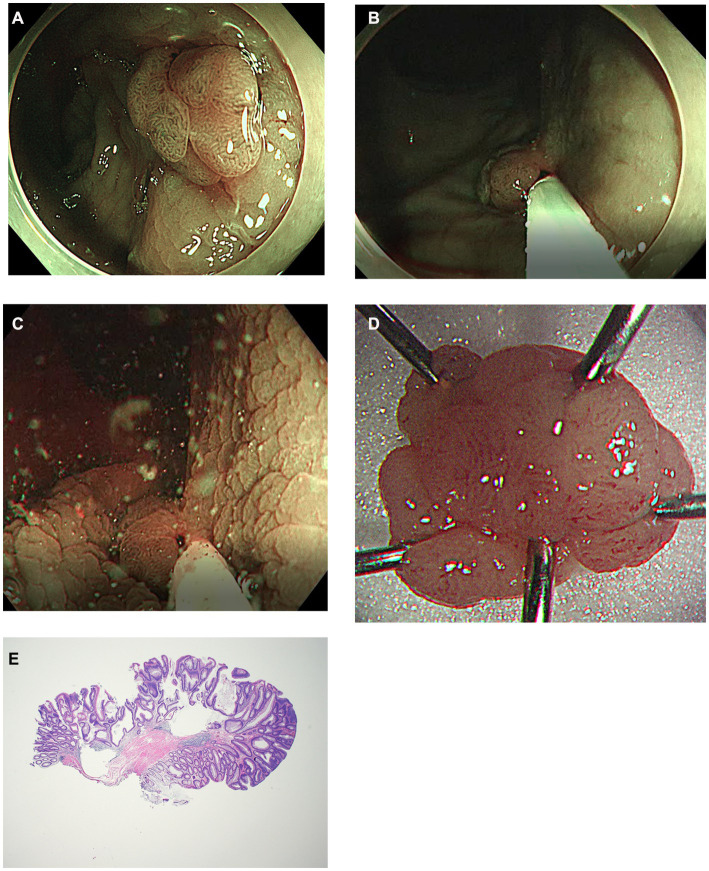
Introduction: Underwater endoscopic mucosal resection (UEMR) is effective for treating intermediate-sized colorectal polyps. However, it is sometimes difficult to obtain visibility in underwater conditions.
Methods: This prospective, observational, single-center study included consecutive patients with intermediate-sized (10-20 mm) sessile colorectal polyps. Modified UEMR method was used to initially snare the lesion without injection or water infusion. Thereafter, water was infused until the lesion was submerged, then it was resected using electrocautery. We also evaluated the rates of complete resection and procedure-related complications.
Results: Forty-two patients with 47 polyps were enrolled in the study. The median procedure time and fluid infusion were 71 s (42-607) and 50 mL (30-130), respectively. The rates of R0 resection and en bloc resection were 80.9 and 97.9%, respectively, with 100% technical success. R0 resection was observed in 42.9% of polyps sized ≥15 mm and 87.5% sized <15 mm (p < 0.01). Muscle entrapment was found in 71.4% of patients with polyps sized ≥15 mm and 10% <15 mm (p < 0.01). Immediate bleeding occurred in 12.8% of cases and was controlled using a snare tip or hemostatic forceps. Snare-tip ablation and hemostatic forceps ablation were performed in 27.7 and 6.4% of patients, respectively. No delayed bleeding, perforation, or any other complications were reported.
Conclusion: Modified UEMR can be used in cases in which securing visibility or performing the existing UEMR is challenging. Careful treatment is required when removing polyps >15 mm in size.
Keywords: colonic polyps; endoscopic mucosal resection; endoscopy; neoplasm (MeSH term); water.
Copyright © 2023 Kim, Park, You, Jung, Joo, Myung, Kim, Kim, Kim and Ju.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials