

The Hypothalamus-pituitary-adrenocortical Response to Critical Illness: A Concept in Need of Revision
- PMID: 37409973
- PMCID: PMC10638597
- DOI: 10.1210/endrev/bnad021
The Hypothalamus-pituitary-adrenocortical Response to Critical Illness: A Concept in Need of Revision
Abstract
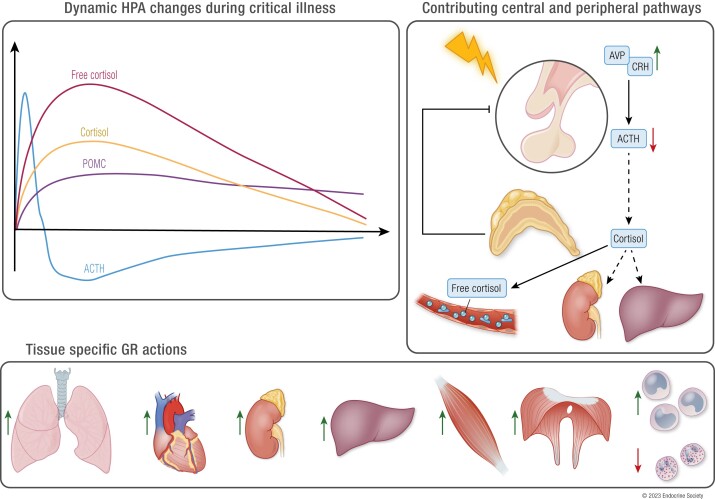
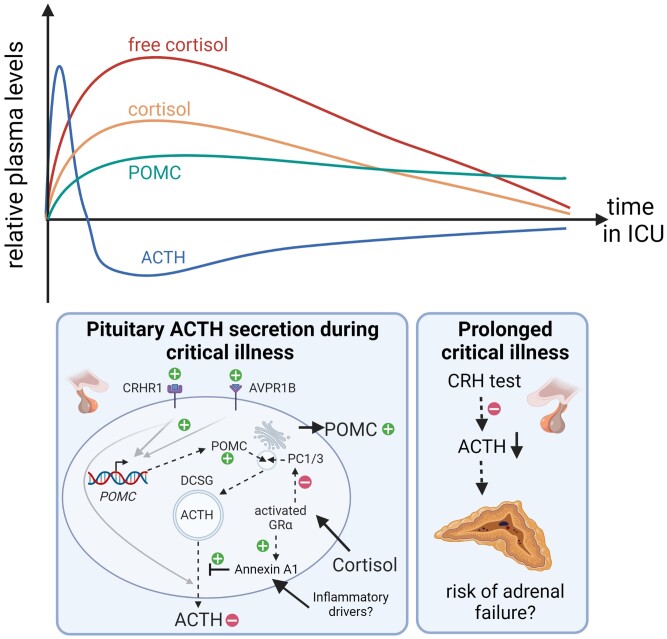
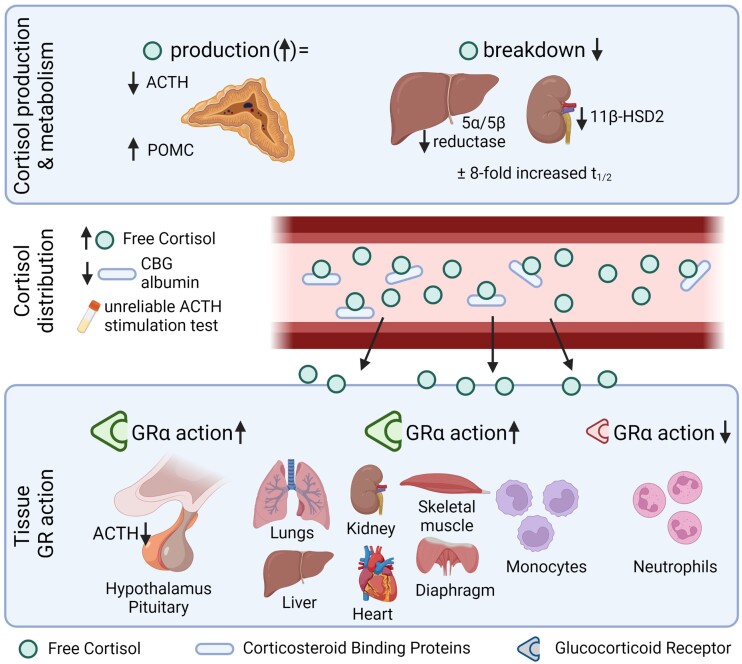
Based on insights obtained during the past decade, the classical concept of an activated hypothalamus-pituitary-adrenocortical axis in response to critical illness is in need of revision. After a brief central hypothalamus-pituitary-adrenocortical axis activation, the vital maintenance of increased systemic cortisol availability and action in response to critical illness is predominantly driven by peripheral adaptations rather than by an ongoing centrally activated several-fold increased production and secretion of cortisol. Besides the known reduction of cortisol-binding proteins that increases free cortisol, these peripheral responses comprise suppressed cortisol metabolism in liver and kidney, prolonging cortisol half-life, and local alterations in expression of 11βHSD1, glucocorticoid receptor-α (GRα), and FK506 binding protein 5 (FKBP51) that appear to titrate increased GRα action in vital organs and tissues while reducing GRα action in neutrophils, possibly preventing immune-suppressive off-target effects of increased systemic cortisol availability. Peripherally increased cortisol exerts negative feed-back inhibition at the pituitary level impairing processing of pro-opiomelanocortin into ACTH, thereby reducing ACTH-driven cortisol secretion, whereas ongoing central activation results in increased circulating pro-opiomelanocortin. These alterations seem adaptive and beneficial for the host in the short term. However, as a consequence, patients with prolonged critical illness who require intensive care for weeks or longer may develop a form of central adrenal insufficiency. The new findings supersede earlier concepts such as "relative," as opposed to "absolute," adrenal insufficiency and generalized systemic glucocorticoid resistance in the critically ill. The findings also question the scientific basis for broad implementation of stress dose hydrocortisone treatment of patients suffering from acute septic shock solely based on assumption of cortisol insufficiency.
Keywords: binding proteins; cortisol; critical illness; glucocorticoid receptor; sepsis.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Similar articles
-
Critical Illness-induced Corticosteroid Insufficiency: What It Is Not and What It Could Be.J Clin Endocrinol Metab. 2022 Jun 16;107(7):2057-2064. doi: 10.1210/clinem/dgac201. J Clin Endocrinol Metab. 2022. PMID: 35358303 Free PMC article. Review.
-
Adrenal function/dysfunction in critically ill patients: a concise narrative review of recent novel insights.J Anesth. 2021 Dec;35(6):903-910. doi: 10.1007/s00540-021-02977-x. Epub 2021 Jul 24. J Anesth. 2021. PMID: 34302540 Review.
-
The hypothalamus-pituitary-adrenal axis in sepsis- and hyperinflammation-induced critical illness: Gaps in current knowledge and future translational research directions.EBioMedicine. 2022 Oct;84:104284. doi: 10.1016/j.ebiom.2022.104284. Epub 2022 Sep 23. EBioMedicine. 2022. PMID: 36162206 Free PMC article. Review.
-
Impact of Hydrocortisone and of CRH Infusion on the Hypothalamus-Pituitary-Adrenocortical Axis of Septic Male Mice.Endocrinology. 2022 Jan 1;163(1):bqab222. doi: 10.1210/endocr/bqab222. Endocrinology. 2022. PMID: 34698826 Free PMC article.
-
New insights into the controversy of adrenal function during critical illness.Lancet Diabetes Endocrinol. 2015 Oct;3(10):805-15. doi: 10.1016/S2213-8587(15)00224-7. Epub 2015 Jun 10. Lancet Diabetes Endocrinol. 2015. PMID: 26071883 Review.
Cited by
-
Effect of methylprednisolone vs hydrocortisone on 30-day mortality in critically ill adults with septic shock: an analysis of the MIMIC-IV database.BMC Infect Dis. 2025 Mar 8;25(1):328. doi: 10.1186/s12879-025-10731-x. BMC Infect Dis. 2025. PMID: 40055601 Free PMC article.
-
Critical illness-related corticosteroid insufficiency (CIRCI) - an overview of pathogenesis, clinical presentation and management.Front Endocrinol (Lausanne). 2024 Nov 6;15:1473151. doi: 10.3389/fendo.2024.1473151. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39574948 Free PMC article. Review.
-
Endocrine Disorders in Critically Ill Patients - The Smooth Criminal?J Crit Care Med (Targu Mures). 2024 Jul 31;10(3):195-197. doi: 10.2478/jccm-2024-0034. eCollection 2024 Jul. J Crit Care Med (Targu Mures). 2024. PMID: 39108412 Free PMC article. No abstract available.
-
Altered muscle transcriptome as molecular basis of long-term muscle weakness in survivors from critical illness.Intensive Care Med. 2025 Jun;51(6):1062-1077. doi: 10.1007/s00134-025-07949-3. Epub 2025 Jun 10. Intensive Care Med. 2025. PMID: 40493222 Free PMC article. Clinical Trial.
-
Diagnosing and treating the elderly individual with hypopituitarism.Rev Endocr Metab Disord. 2024 Jun;25(3):575-597. doi: 10.1007/s11154-023-09870-w. Epub 2023 Dec 27. Rev Endocr Metab Disord. 2024. PMID: 38150092 Review.
References
-
- Nates JL, Nunnally M, Kleinpell R, et al. . ICU admission, discharge, and triage guidelines: a framework to enhance clinical operations, development of institutional policies, and further research. Crit Care Med. 2016;44(8):1553‐1602. - PubMed
-
- Iwashyna TJ, Hodgson CL, Pilcher D, et al. . Timing of onset and burden of persistent critical illness in Australia and New Zealand: a retrospective, population-based, observational study. Lancet Respir Med. 2016;4(7):566‐573. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
