

CDK4/6-MEK Inhibition in MPNSTs Causes Plasma Cell Infiltration, Sensitization to PD-L1 Blockade, and Tumor Regression
- PMID: 37410426
- PMCID: PMC10528807
- DOI: 10.1158/1078-0432.CCR-23-0749
CDK4/6-MEK Inhibition in MPNSTs Causes Plasma Cell Infiltration, Sensitization to PD-L1 Blockade, and Tumor Regression
Abstract
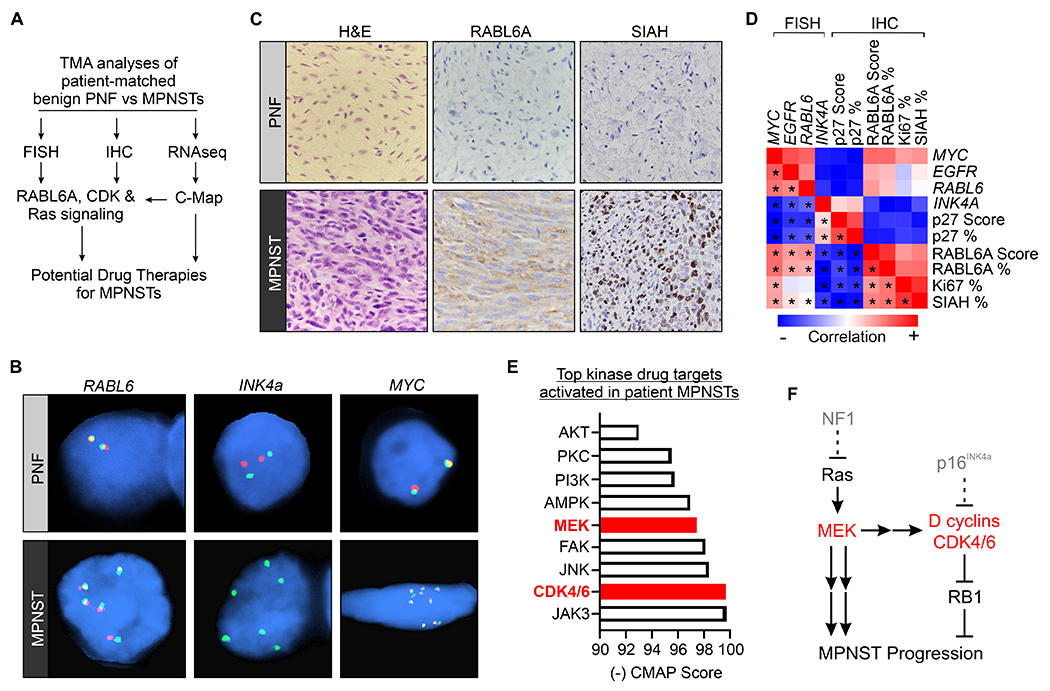
Purpose: Malignant peripheral nerve sheath tumors (MPNST) are lethal, Ras-driven sarcomas that lack effective therapies. We investigated effects of targeting cyclin-dependent kinases 4 and 6 (CDK4/6), MEK, and/or programmed death-ligand 1 (PD-L1) in preclinical MPNST models.
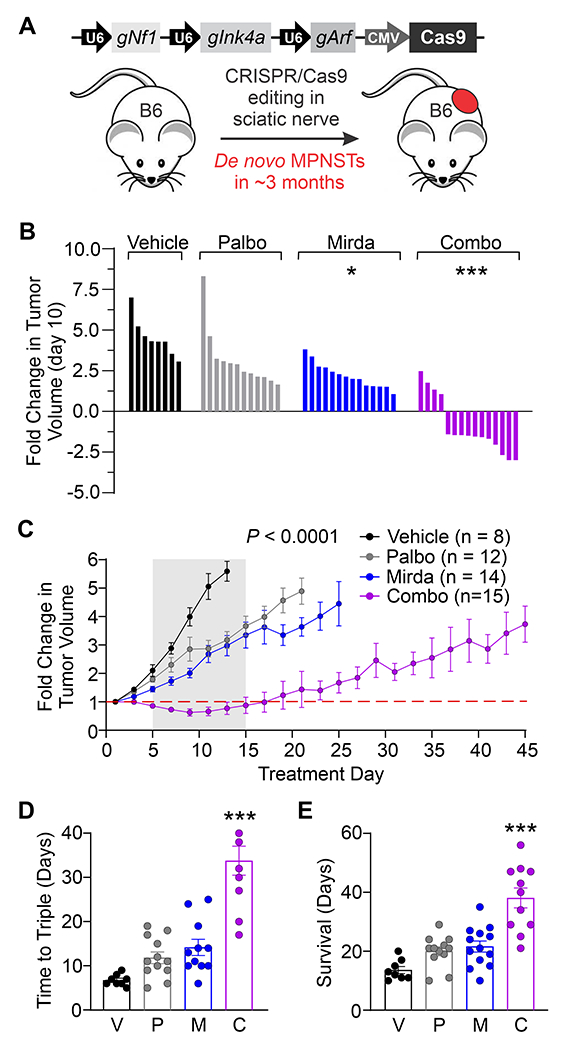
Experimental design: Patient-matched MPNSTs and precursor lesions were examined by FISH, RNA sequencing, IHC, and Connectivity-Map analyses. Antitumor activity of CDK4/6 and MEK inhibitors was measured in MPNST cell lines, patient-derived xenografts (PDX), and de novo mouse MPNSTs, with the latter used to determine anti-PD-L1 response.
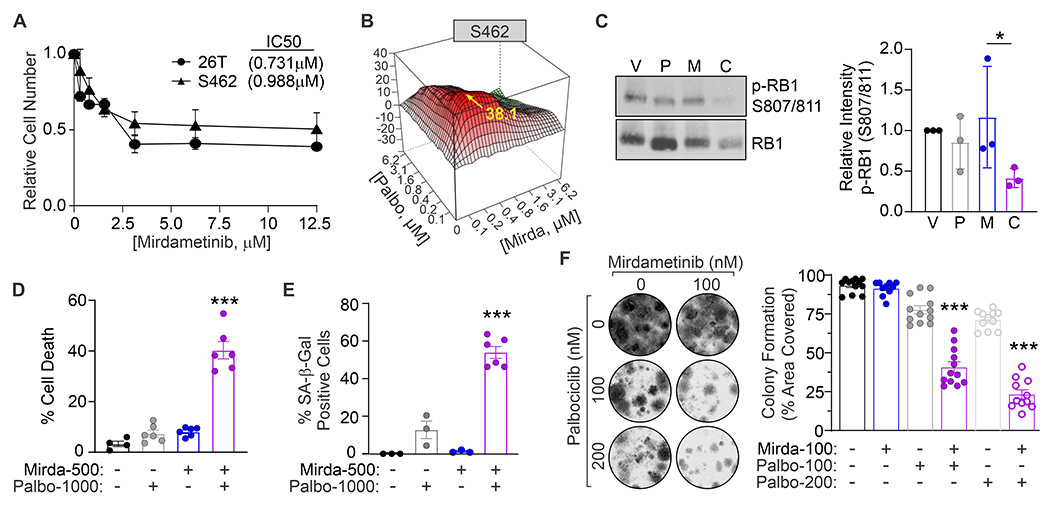
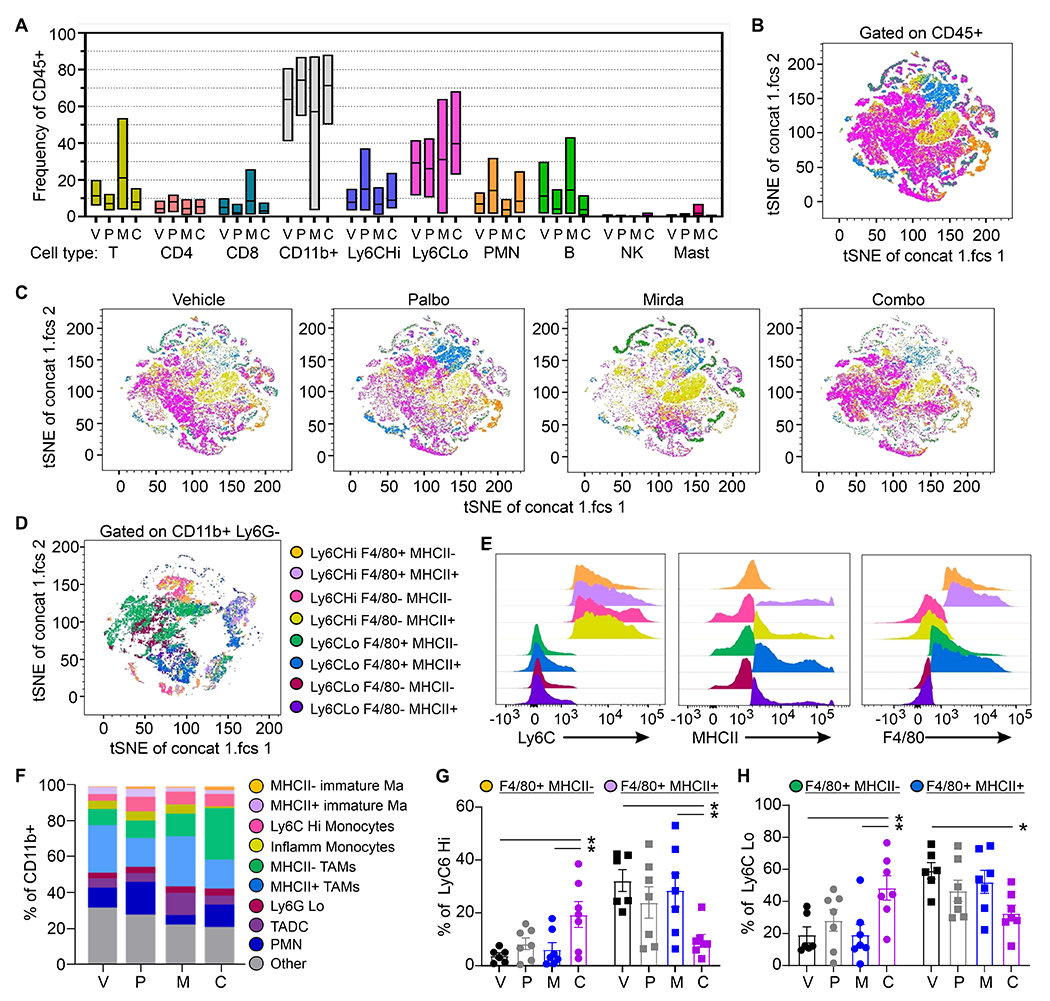
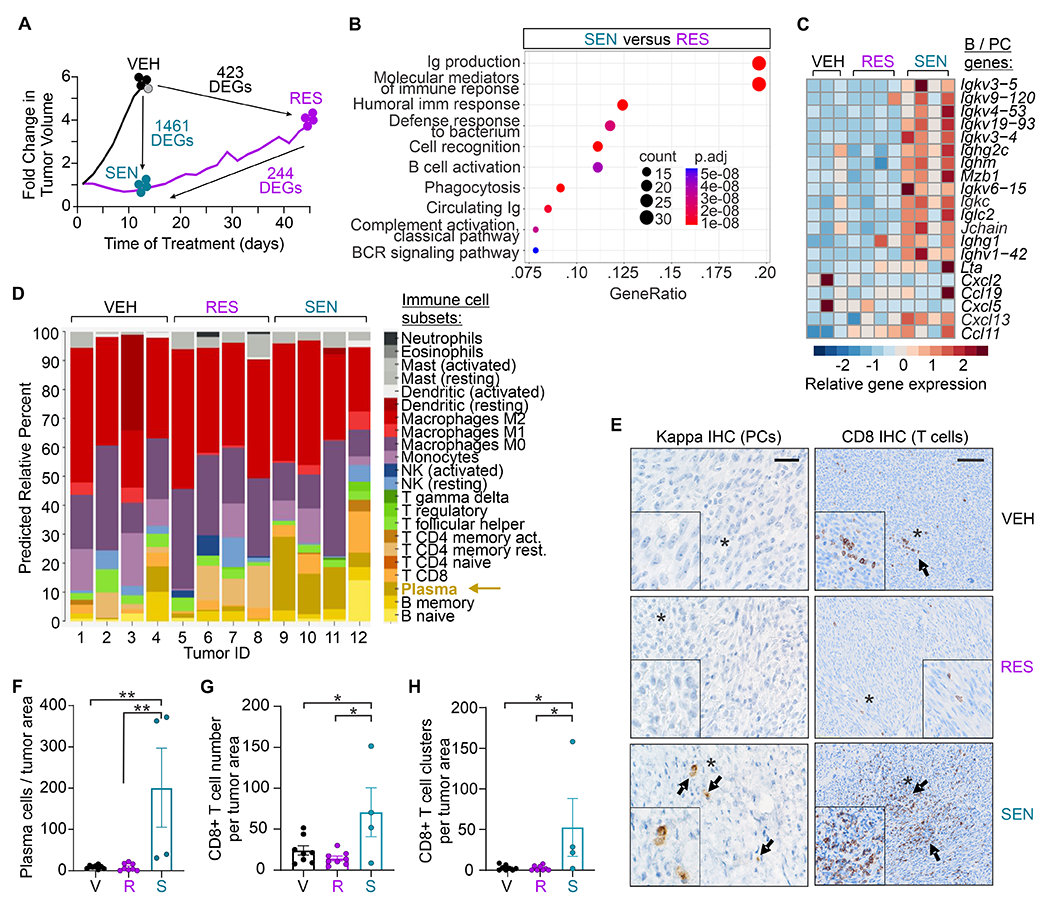
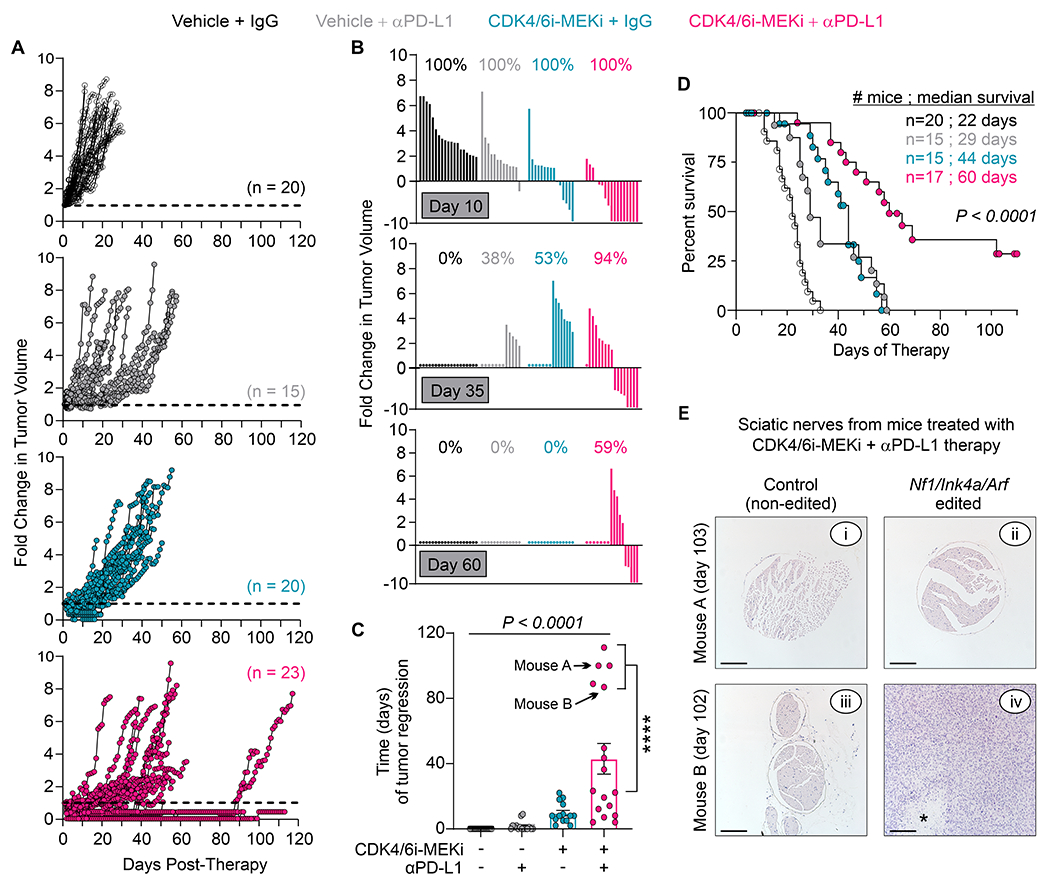
Results: Patient tumor analyses identified CDK4/6 and MEK as actionable targets for MPNST therapy. Low-dose combinations of CDK4/6 and MEK inhibitors synergistically reactivated the retinoblastoma (RB1) tumor suppressor, induced cell death, and decreased clonogenic survival of MPNST cells. In immune-deficient mice, dual CDK4/6-MEK inhibition slowed tumor growth in 4 of 5 MPNST PDXs. In immunocompetent mice, combination therapy of de novo MPNSTs caused tumor regression, delayed resistant tumor outgrowth, and improved survival relative to monotherapies. Drug-sensitive tumors that regressed contained plasma cells and increased cytotoxic T cells, whereas drug-resistant tumors adopted an immunosuppressive microenvironment with elevated MHC II-low macrophages and increased tumor cell PD-L1 expression. Excitingly, CDK4/6-MEK inhibition sensitized MPNSTs to anti-PD-L1 immune checkpoint blockade (ICB) with some mice showing complete tumor regression.
Conclusions: CDK4/6-MEK inhibition induces a novel plasma cell-associated immune response and extended antitumor activity in MPNSTs, which dramatically enhances anti-PD-L1 therapy. These preclinical findings provide strong rationale for clinical translation of CDK4/6-MEK-ICB targeted therapies in MPNST as they may yield sustained antitumor responses and improved patient outcomes.
©2023 American Association for Cancer Research.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
