

Efficacy of immune checkpoint inhibitors for the treatment of advanced melanoma in patients with concomitant chronic lymphocytic leukemia
- PMID: 37414216
- PMCID: PMC11289780
- DOI: 10.1016/j.annonc.2023.06.007
Efficacy of immune checkpoint inhibitors for the treatment of advanced melanoma in patients with concomitant chronic lymphocytic leukemia
Abstract
Background: Immune checkpoint inhibitors (ICIs) have revolutionized the management of advanced melanoma (AM). However, data on ICI effectiveness have largely been restricted to clinical trials, thereby excluding patients with co-existing malignancies. Chronic lymphocytic leukemia (CLL) is the most prevalent adult leukemia and is associated with increased risk of melanoma. CLL alters systemic immunity and can induce T-cell exhaustion, which may limit the efficacy of ICIs in patients with CLL. We, therefore, sought to examine the efficacy of ICI in patients with these co-occurring diagnoses.
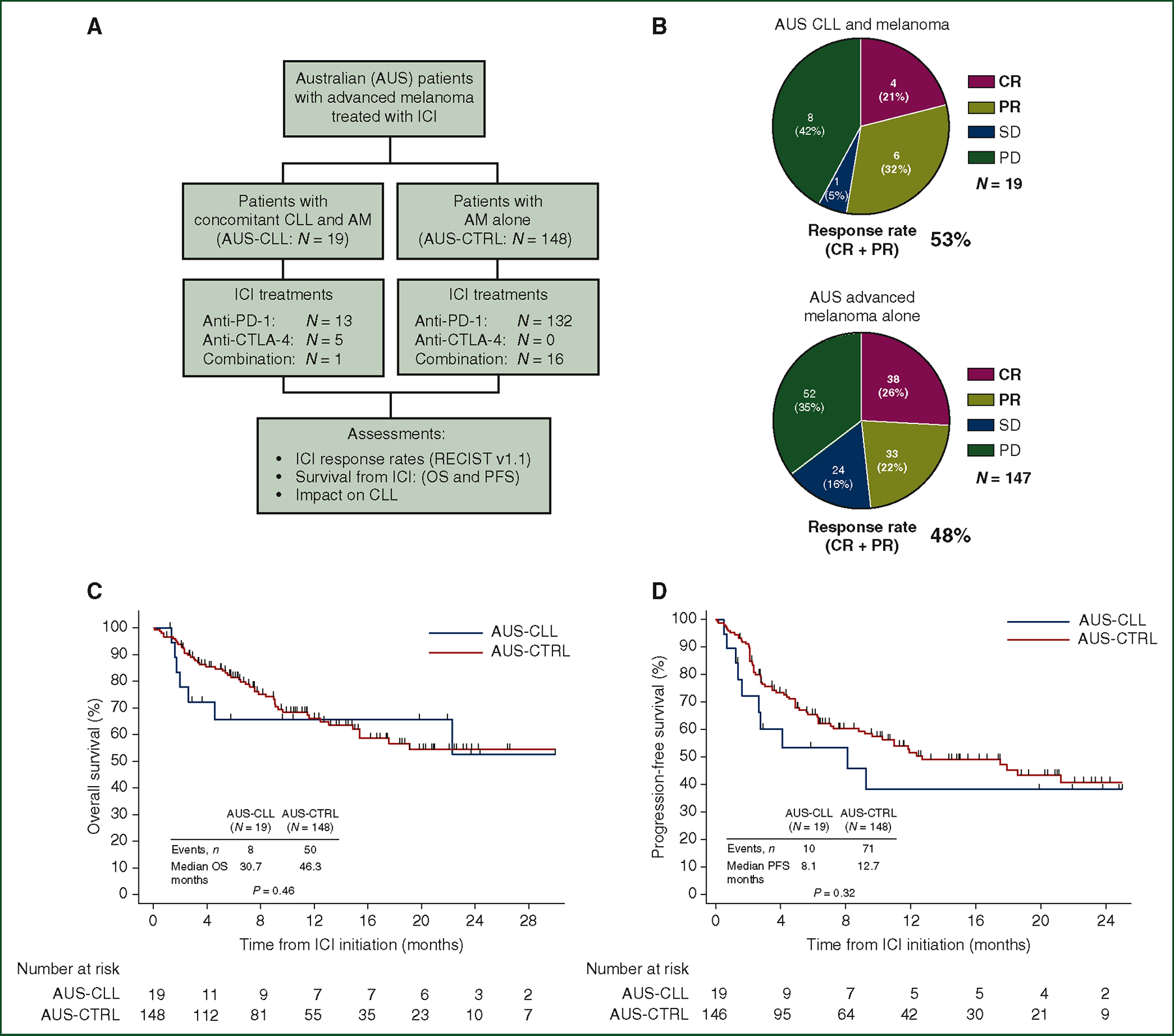
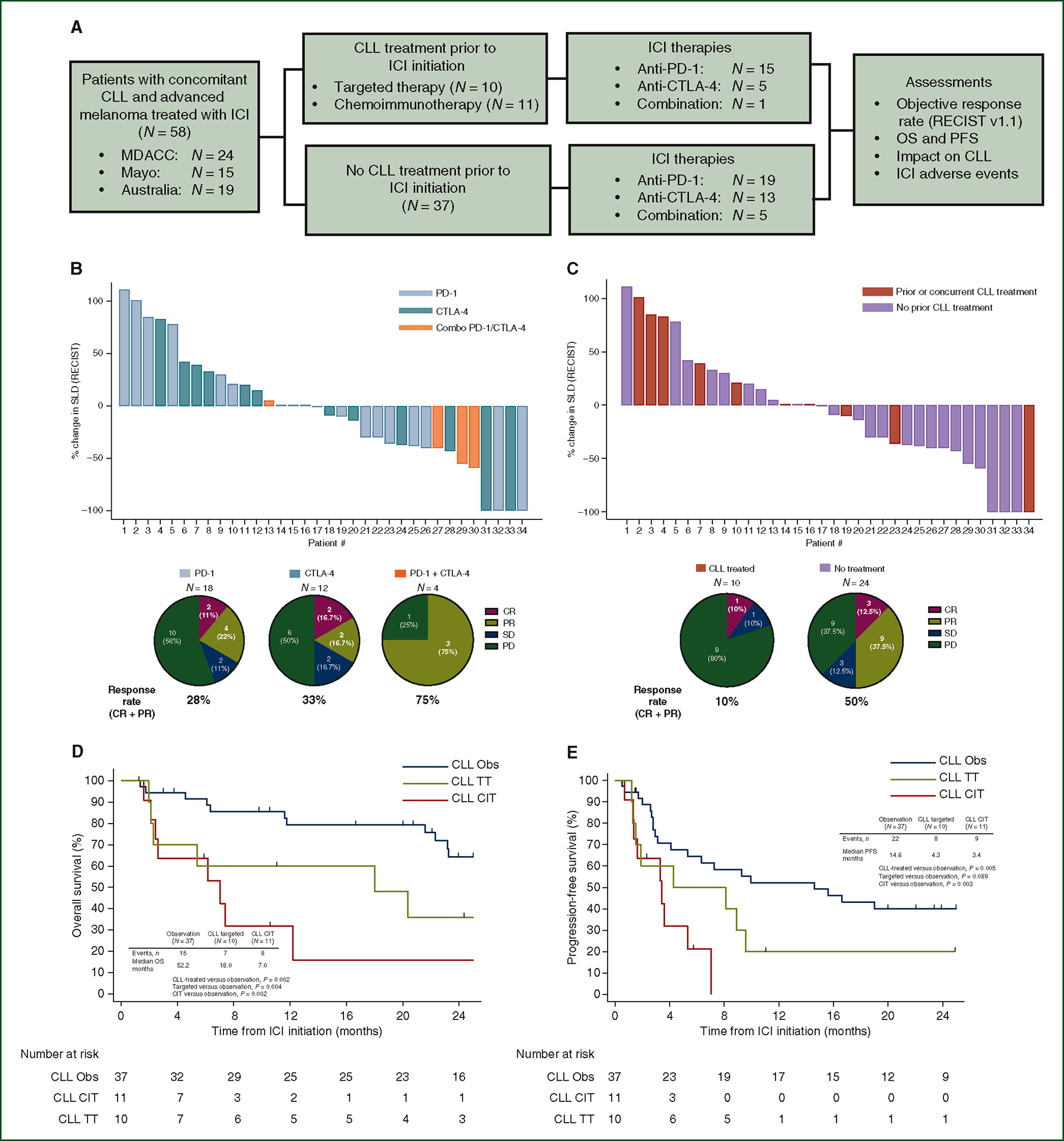
Patients and methods: In this international multicenter study, a retrospective review of clinical databases identified patients with concomitant diagnoses of CLL and AM treated with ICI (US-MD Anderson Cancer Center, N = 24; US-Mayo Clinic, N = 15; AUS, N = 19). Objective response rates (ORRs), assessed by RECIST v1.1, and survival outcomes [overall survival (OS) and progression-free survival (PFS)] among patients with CLL and AM were assessed. Clinical factors associated with improved ORR and survival were explored. Additionally, ORR and survival outcomes were compared between the Australian CLL/AM cohort and a control cohort of 148 Australian patients with AM alone.
Results: Between 1997 and 2020, 58 patients with concomitant CLL and AM were treated with ICI. ORRs were comparable between AUS-CLL/AM and AM control cohorts (53% versus 48%, P = 0.81). PFS and OS from ICI initiation were also comparable between cohorts. Among CLL/AM patients, a majority were untreated for their CLL (64%) at the time of ICI. Patients with prior history of chemoimmunotherapy treatment for CLL (19%) had significantly reduced ORRs, PFS, and OS.
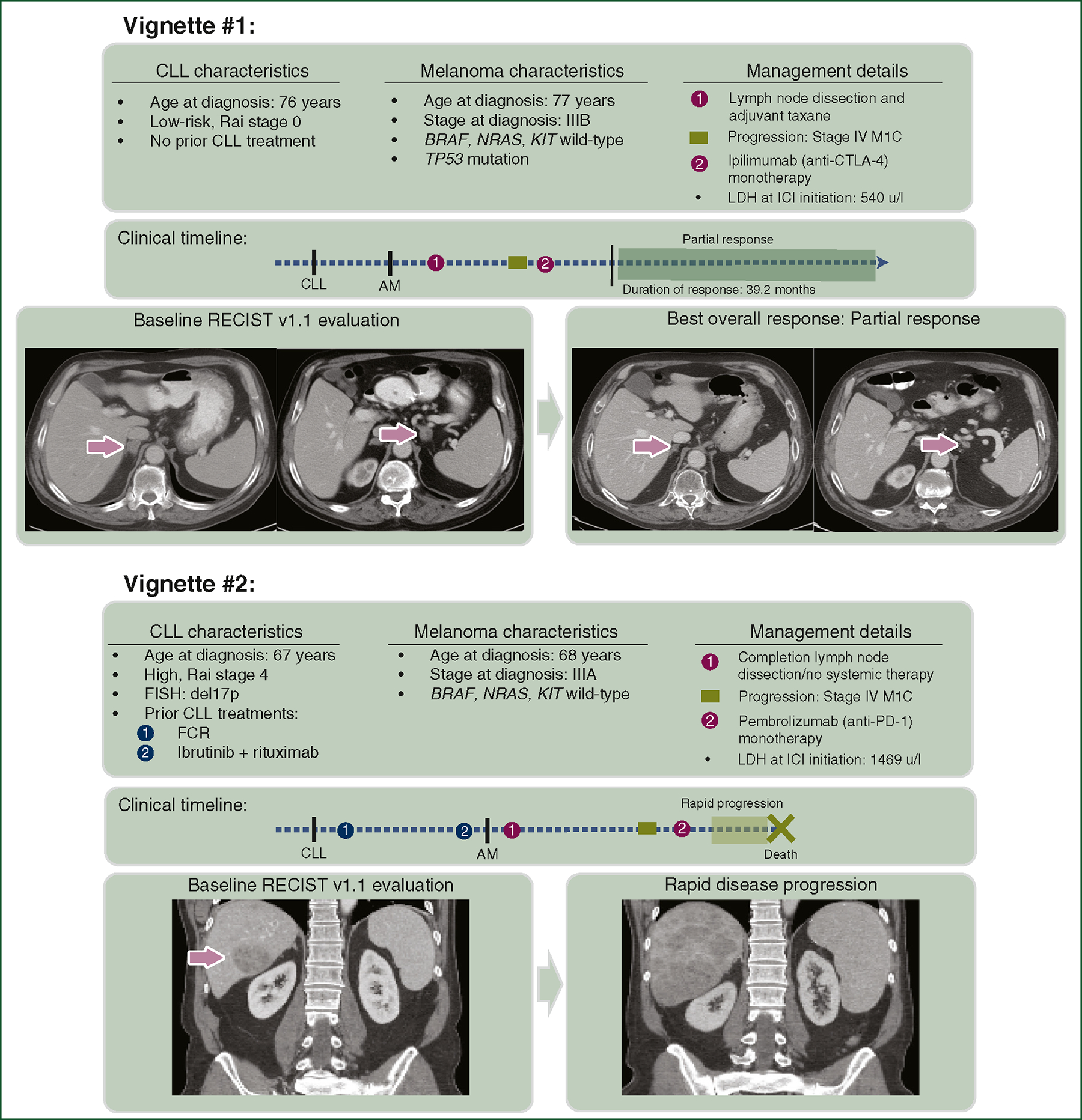
Conclusions: Our case series of patients with concomitant CLL and melanoma demonstrate frequent, durable clinical responses to ICI. However, those with prior chemoimmunotherapy treatment for CLL had significantly worse outcomes. We found that CLL disease course is largely unchanged by treatment with ICI.
Keywords: anti-CTLA-4; anti-PD-1; chronic lymphoid leukemia; immune checkpoint inhibitors; melanoma.
Copyright © 2023 European Society for Medical Oncology. All rights reserved.
Conflict of interest statement
Disclosure JAW is an inventor on a US patent application (PCT/US17/53.717); reports compensation for speaker’s bureau and honoraria from Imedex, Dava Oncology, Omniprex, Illumina, Gilead, PeerView, MedImmune, and Bristol-Myers Squibb (BMS); serves as a consultant/advisory board member for Roche/Genentech, Novartis, AstraZeneca, GlaxoSmithKline (GSK), BMS, Merck, Biothera Pharmaceuticals, and Micronoma. JAW holds stock options from Micronoma. JLM serves as a consultant for Merck and in advisory board for Bristol-Myers Squibb. GVL is a consultant advisor for Agenus, Amgen, Array Biopharma, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Evaxion, Hexal AG (Sandoz Company), Highlight Therapeutics S.L., Innovent Biologics USA, Merck Sharpe & Dohme, Novartis, OncoSec, PHMR Ltd., Pierre Fabre, Provectus, Qbiotics, Regeneron. LW is an advisory board consultant/advisor for Novartis, Merck Sharp and Dohme, and Bristol-Myers Squibb. All other authors have declared no conflicts of interest. Data Sharing The data that support the findings of this study are available from the corresponding author on reasonable request. Role of the Funder/Sponsor The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Figures
References
-
- Eichhorst B, Robak T, Montserrat E, et al. Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32:23–33. - PubMed
-
- Hallek M, Shanafelt TD, Eichhorst B. Chronic lymphocytic leukaemia. Lancet. 2018;391:1524–1537. - PubMed
-
- Solomon BM, Rabe KG, Slager SL, et al. Overall and cancer-specific survival of patients with breast, colon, kidney, and lung cancers with and without chronic lymphocytic leukemia: a SEER population-based study. J Clin Oncol. 2013;31:930–937. - PubMed
-
- Olsen CM, Lane SW, Green AC. Increased risk of melanoma in patients with chronic lymphocytic leukaemia: systematic review and meta-analysis of cohort studies. Melanoma Res. 2016;26:188–194. - PubMed
-
- Brewer JD, Christenson LJ, Weenig RH, Weaver AL. Effects of chronic lymphocytic leukemia on the development and progression of malignant melanoma. Dermatol Surg. 2010;36:368–376. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
