

Coronary artery calcium score and pre-test probabilities as gatekeepers to predict and rule out perfusion defects in positron emission tomography
- PMID: 37415007
- PMCID: PMC10682222
- DOI: 10.1007/s12350-023-03322-3
Coronary artery calcium score and pre-test probabilities as gatekeepers to predict and rule out perfusion defects in positron emission tomography
Abstract
Background: Little is known about the gatekeeper performance of coronary artery calcium score (CACS) before myocardial perfusion positron emission tomography (PET), compared with updated pre-test probabilities from American and European guidelines (pre-test-AHA/ACC, pre-test-ESC).
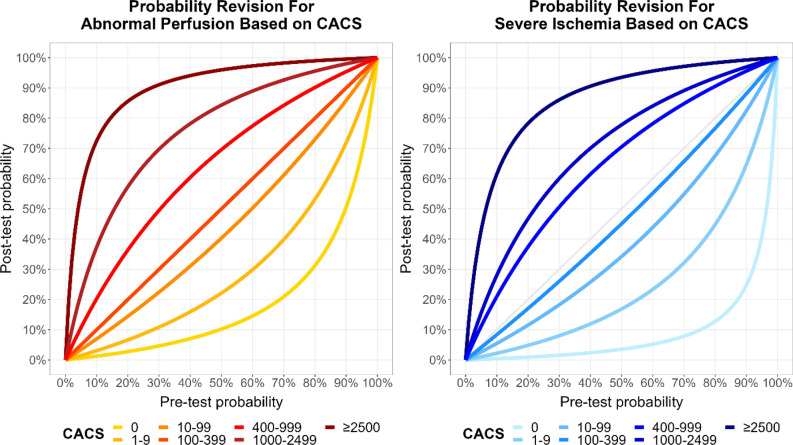
Methods: We enrolled participants without known coronary artery disease undergoing CACS and Rubidium-82 PET. Abnormal perfusion was defined as summed stress score ≥ 4. Using Bayes' formula, pre-test probabilities and CACS were combined into post-test probabilities.
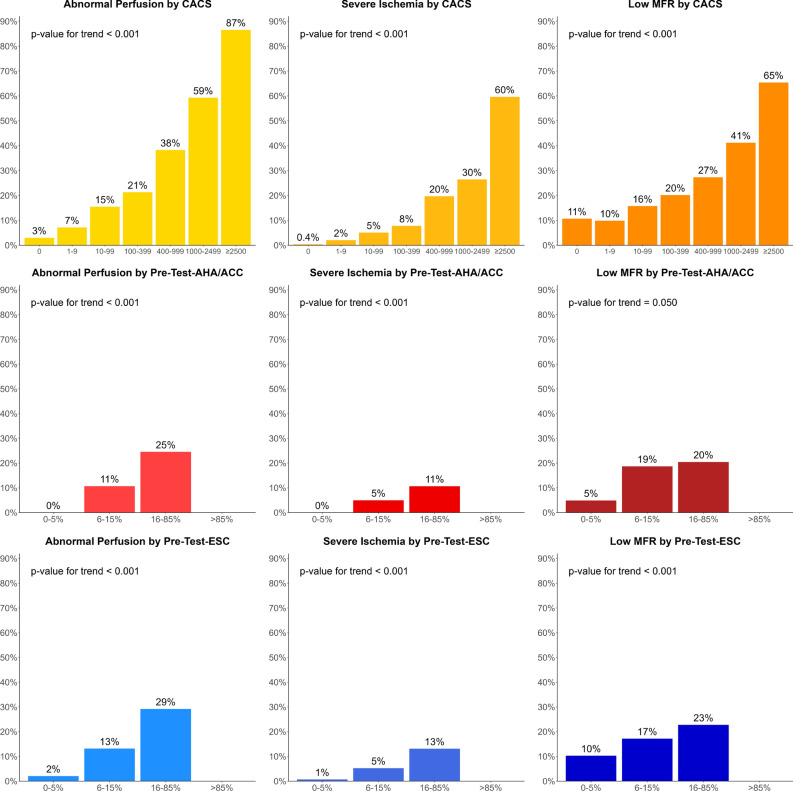
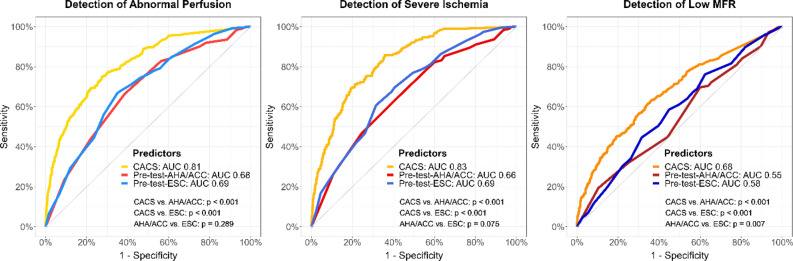
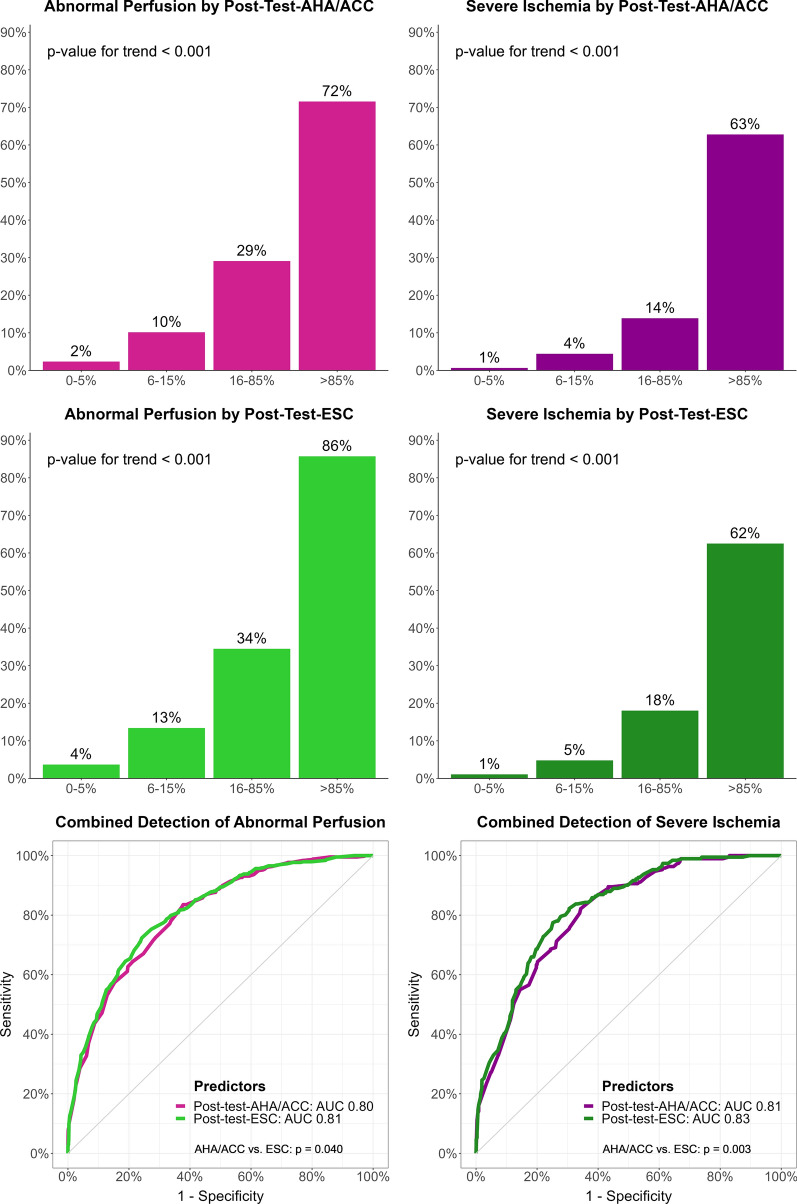
Results: We included 2050 participants (54% male, mean age 64.6 years) with median CACS 62 (IQR 0-380), pre-test-ESC 17% (11-26), pre-test-AHA/ACC 27% (16-44), and abnormal perfusion in 437 participants (21%). To predict abnormal perfusion, area under the curve of CACS was 0.81, pre-test-AHA/ACC 0.68, pre-test-ESC 0.69, post-test-AHA/ACC 0.80, and post-test-ESC 0.81 (P < 0.001 for CACS vs. each pre-test, and each post-test vs. pre-test). CACS = 0 had 97% negative predictive value (NPV), pre-test-AHA/ACC ≤ 5% 100%, pre-test-ESC ≤ 5% 98%, post-test-AHA/ACC ≤ 5% 98%, and post-test-ESC ≤ 5% 96%. Among participants, 26% had CACS = 0, 2% pre-test-AHA/ACC ≤ 5%, 7% pre-test-ESC ≤ 5%, 23% post-test-AHA/ACC ≤ 5%, and 33% post-test-ESC ≤ 5% (all P < 0.001).
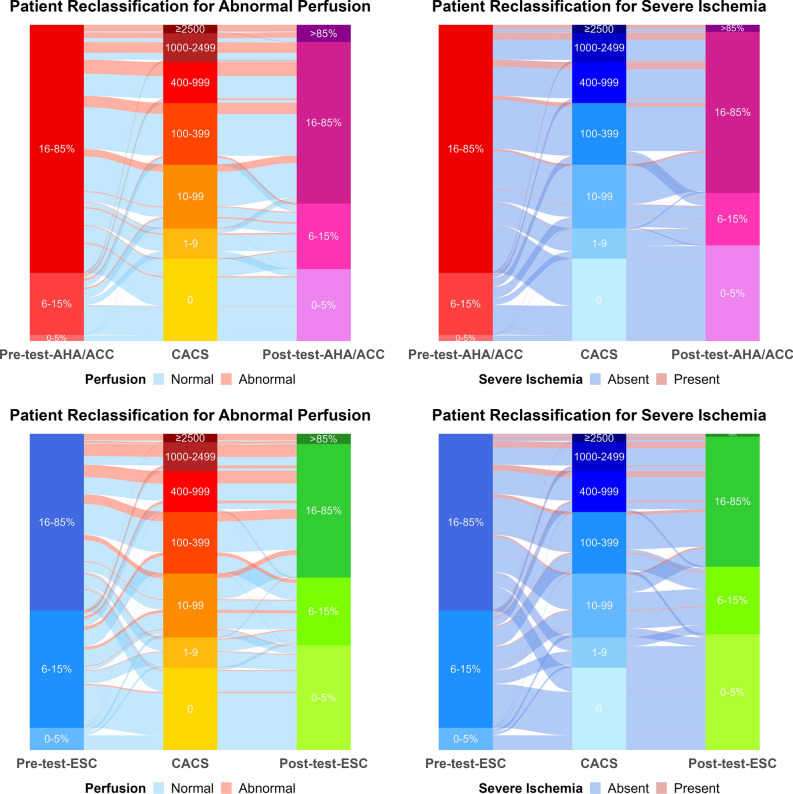
Conclusions: CACS and post-test probabilities are excellent predictors of abnormal perfusion and can rule it out with very high NPV in a substantial proportion of participants. CACS and post-test probabilities may be used as gatekeepers before advanced imaging. Coronary artery calcium score (CACS) predicted abnormal perfusion (SSS ≥ 4) in myocardial positron emission tomography (PET) better than pre-test probabilities of coronary artery disease (CAD), while pre-test-AHA/ACC and pre-test-ESC performed similarly (left). Using Bayes' formula, pre-test-AHA/ACC or pre-test-ESC were combined with CACS into post-test probabilities (middle). This calculation reclassified a substantial proportion of participants to low probability of CAD (0-5%), not needing further imaging, as shown for AHA/ACC probabilities (2% with pre-test-AHA/ACC to 23% with post-test-AHA/ACC, P < 0.001, right). Very few participants with abnormal perfusion were classified under pre-test or post-test probabilities 0-5%, or under CACS 0. AUC: area under the curve. Pre-test-AHA/ACC: Pre-test probability of the American Heart Association/American College of Cardiology. Post-test-AHA/ACC: Post-test probability combining pre-test-AHA/ACC and CACS. Pre-test-ESC: Pre-test probability of the European Society of Cardiology. SSS: Summed stress score.
© 2023. The Author(s).
Conflict of interest statement
Olivier F Clerc, Simon M Frey, Ursina Honegger, Melissa LF Amrein, Federico Caobelli, Philip Haaf and Michael J Zellweger: No conflict of interest related to this study. This study received no funding.
Figures
Comment in
-
Coronary artery calcium score as a gatekeeper: are we there yet?J Nucl Cardiol. 2023 Dec;30(6):2574-2577. doi: 10.1007/s12350-023-03368-3. Epub 2023 Sep 12. J Nucl Cardiol. 2023. PMID: 37700214 No abstract available.
References
-
- Institute for Health Metrics and Evaluation (IHME). GBD 2019 Cause and Risk Summary: Ischaemic heart disease—Level 3 cause. Seattle, USA; 2019.
-
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144:e368–e454. - PubMed
-
- Schenker MP, Dorbala S, Hong EC, Rybicki FJ, Hachamovitch R, Kwong RY, et al. Interrelation of coronary calcification, myocardial ischemia, and outcomes in patients with intermediate likelihood of coronary artery disease: a combined positron emission tomography/computed tomography study. Circulation. 2008;117:1693–1700. doi: 10.1161/CIRCULATIONAHA.107.717512. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
