

Lessons Learned from Telemonitoring in an Outpatient Bariatric Surgery Pathway-Secondary Outcomes of a Patient Preference Clinical Trial
- PMID: 37415024
- PMCID: PMC10435410
- DOI: 10.1007/s11695-023-06637-9
Lessons Learned from Telemonitoring in an Outpatient Bariatric Surgery Pathway-Secondary Outcomes of a Patient Preference Clinical Trial
Abstract
Background: Remote monitoring is increasingly used to support postoperative care. This study aimed to describe the lessons learned from the use of telemonitoring in an outpatient bariatric surgery pathway.
Materials and methods: Patients were assigned based on their preference to an intervention cohort of same-day discharge after bariatric surgery. In total, 102 patients were monitored continuously for 7 days using a wearable monitoring device with a Continuous and Remote Early Warning Score-based notification protocol (CREWS). Outcome measures included missing data, course of postoperative heart and respiration rate, false positive notification and specificity analysis, and vital sign assessment during teleconsultation.
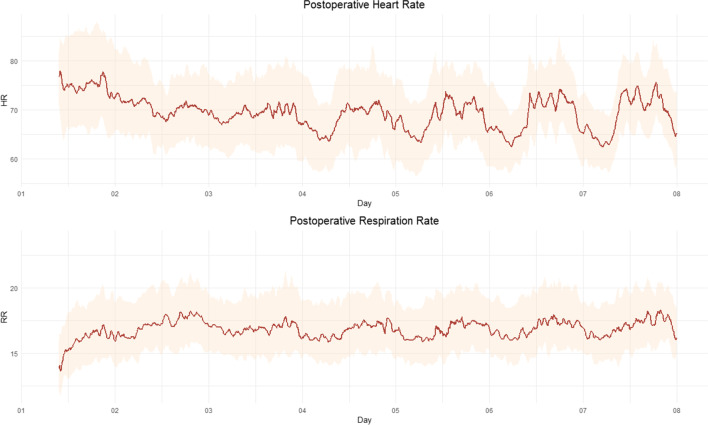
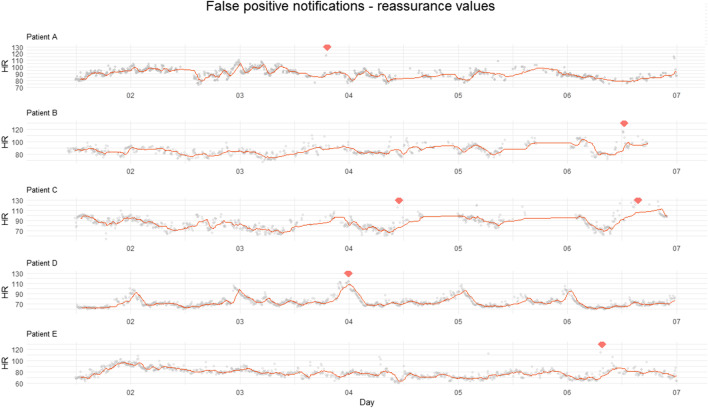
Results: In 14.7% of the patients, data for heart rate was missing for > 8 h. A day-night-rhythm of heart rate and respiration rate reappeared on average on postoperative day 2 with heart rate amplitude increasing after day 3. CREWS notification had a specificity of 98%. Of the 17 notifications, 70% was false positive. Half of them occurred between day 4 and 7 and were accompanied with surrounding reassuring values. Comparable postoperative complaints were encountered between patients with normal and deviated data.
Conclusion: Telemonitoring after outpatient bariatric surgery is feasible. It supports clinical decisions, however does not replace nurse or physician care. Although infrequent, the false notification rate was high. We suggested additional contact may not be necessary when notifications occur after restoration of circadian rhythm or when surrounding reassuring vital signs are present. CREWS supports ruling out serious complications, what may reduce in-hospital re-evaluations. Following these lessons learned, increased patients' comfort and decreased clinical workload could be expected.
Trial registration: ClinicalTrials.gov. Identifier: NCT04754893.
Keywords: Clinical practice; Continuous and remote monitoring; Outpatient bariatric surgery; Telemonitoring.
© 2023. The Author(s).
Conflict of interest statement
The authors E.S. van Ede, J. Scheerhoorn, F.M.J.F. Schonck, J.A van der Stam, and M.P. Buise have no potential conflicts of interest to declare. S.W. Nienhuijs receives an educational grant from Medtronic to the obesity center and R.A. Bouwman acts as a clinical consultant for Philips Research.
Figures


References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
