

Genotype and clinical characteristics of patients with Wolfram syndrome and WFS1-related disorders
- PMID: 37415600
- PMCID: PMC10321297
- DOI: 10.3389/fgene.2023.1198171
Genotype and clinical characteristics of patients with Wolfram syndrome and WFS1-related disorders
Abstract
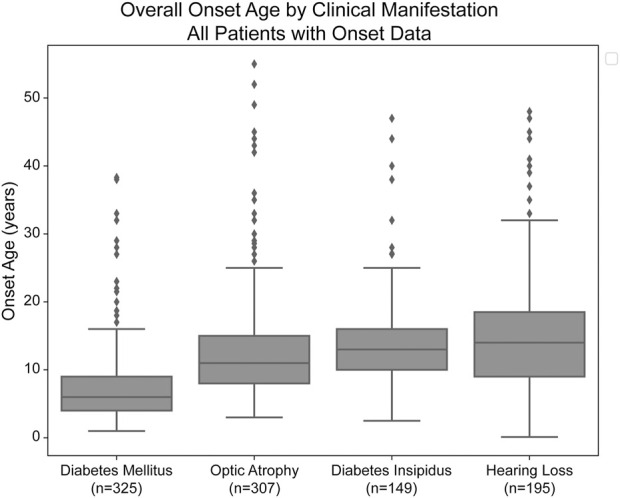
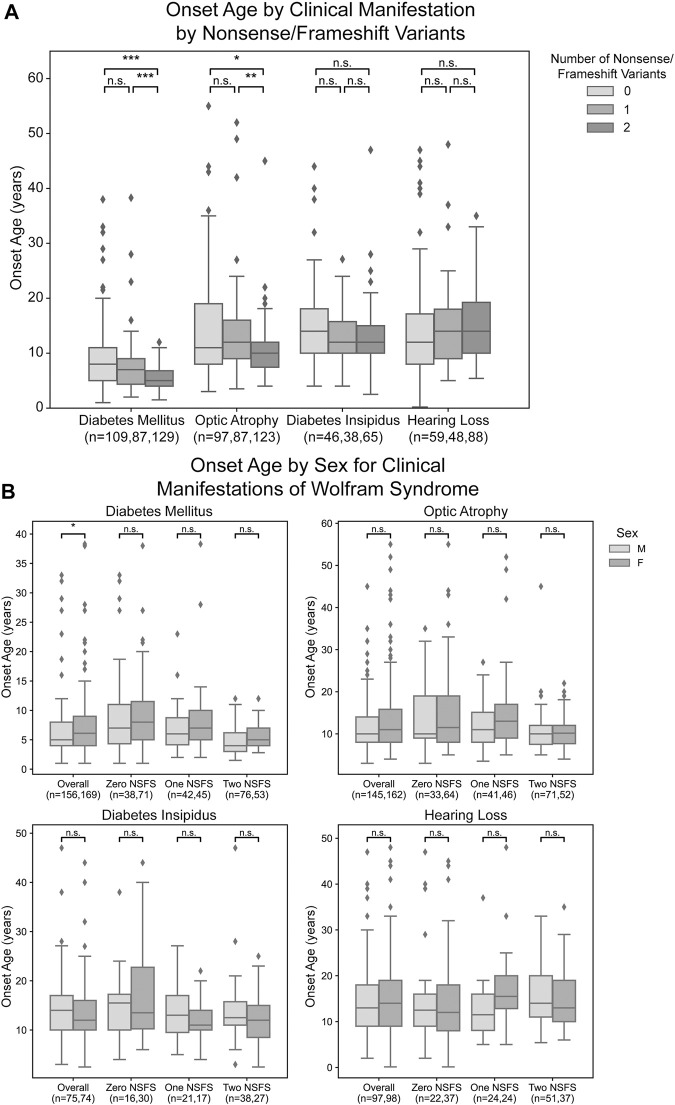
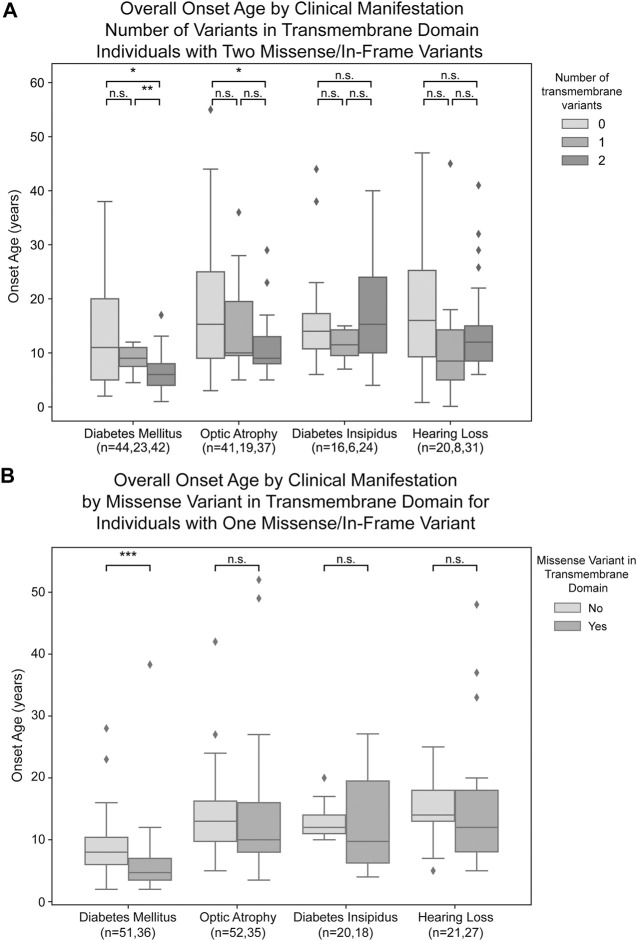
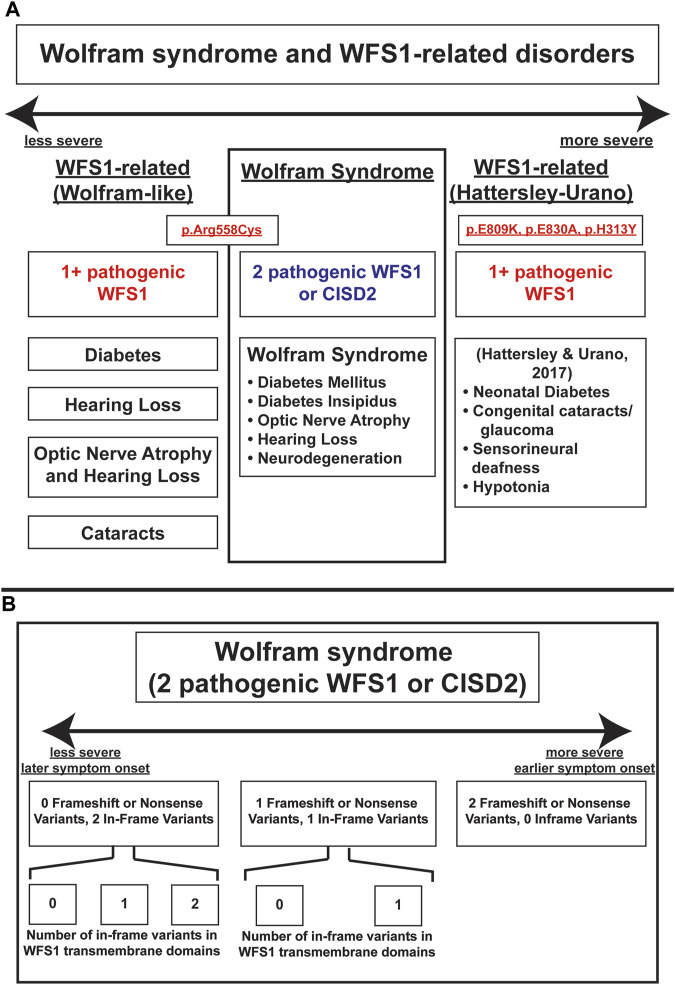
Objective: Wolfram syndrome (WFS) is an autosomal recessive disorder associated with juvenile-onset diabetes mellitus, optic atrophy, diabetes insipidus, and sensorineural hearing loss. We sought to elucidate the relationship between genotypic and phenotypic presentations of Wolfram syndrome which would assist clinicians in classifying the severity and prognosis of Wolfram syndrome more accurately. Approach: Patient data from the Washington University International Registry and Clinical Study for Wolfram Syndrome and patient case reports were analyzed to select for patients with two recessive mutations in the WFS1 gene. Mutations were classified as being either nonsense/frameshift variants or missense/in-frame insertion/deletion variants. Missense/in-frame variants were further classified as transmembrane or non-transmembrane based on whether they affected amino acid residues predicted to be in transmembrane domains of WFS1. Statistical analysis was performed using Wilcoxon rank-sum tests with multiple test adjustment applied via the Bonferonni correction. Results: A greater number of genotype variants correlated with earlier onset and a more severe presentation of Wolfram syndrome. Secondly, non-sense and frameshift variants had more severe phenotypic presentations than missense variants, as evidenced by diabetes mellitus and optic atrophy emerging significantly earlier in patients with two nonsense/frameshift variants compared with zero or one nonsense/frameshift variants. In addition, the number of transmembrane in-frame variants demonstrated a statistically significant dose-effect on age of onset of diabetes mellitus and optic atrophy among patients with either one or two in-frame variants. Summary/Conclusion: The results contribute to our current understanding of the genotype-phenotype relationship of Wolfram syndrome, suggesting that alterations in coding sequences result in significant changes in the presentation and severity of Wolfram. The impact of these findings is significant, as the results will aid clinicians in predicting more accurate prognoses and pave the way for personalized treatments for Wolfram syndrome.
Keywords: WFS1-related disorders; diabetes insipidus; diabetes mellitus; genotype phenotype correlation; hearing loss; optic atrophy; wolfram syndrome.
Copyright © 2023 Lee, Verma, Palaniappan, Pope, Lee, Blacher, Neerumalla, An, Campbell, Brown, Hurst, Marshall, Hershey, Nunes, López de Heredia and Urano.
Conflict of interest statement
FU is an inventor of three patents related to the treatment of wolfram syndrome, us 9,891,231 soluble manf in pancreatic beta cell disorders and us 10,441,574 and us 10,695,324 treatment for wolfram syndrome and other ER stress disorders. FU is a founder and president of CURE4WOLFRAM, INC., and a chair of the scientific advisory board for opris biotechnologies. FU receives research funding from both prilenia and amylyx pharmaceuticals that are developing novel treatments for neurodegenerative disorders, including wolfram syndrome. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Update of
-
Genotype and Clinical Characteristics of Patients with Wolfram Syndrome and WFS1-related Disorders.medRxiv [Preprint]. 2023 Feb 16:2023.02.15.23284904. doi: 10.1101/2023.02.15.23284904. medRxiv. 2023. Update in: Front Genet. 2023 Jun 21;14:1198171. doi: 10.3389/fgene.2023.1198171. PMID: 36824811 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources