

Iron-Deficiency Anemia in CKD: A Narrative Review for the Kidney Care Team
- PMID: 37415621
- PMCID: PMC10319843
- DOI: 10.1016/j.xkme.2023.100677
Iron-Deficiency Anemia in CKD: A Narrative Review for the Kidney Care Team
Abstract
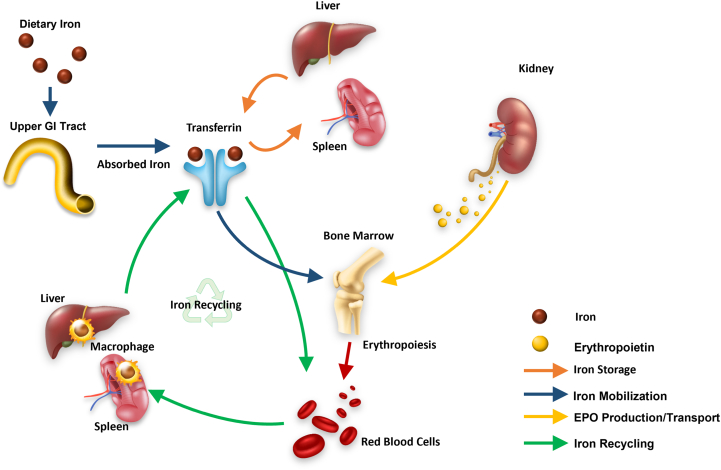
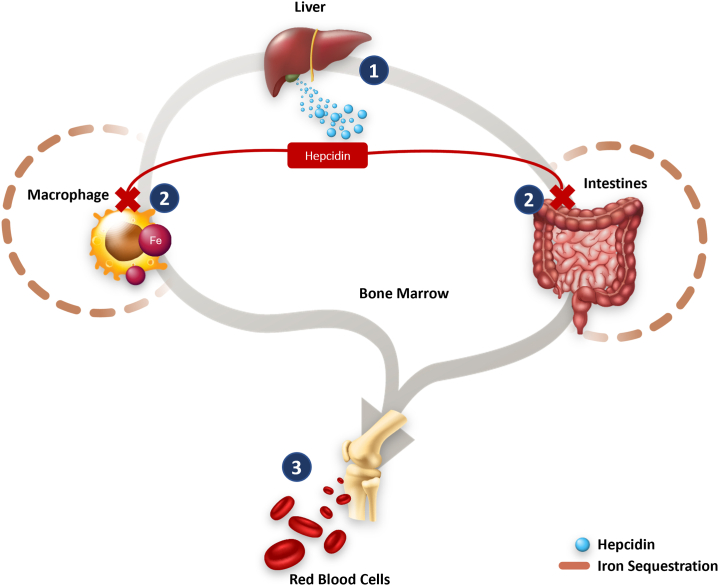
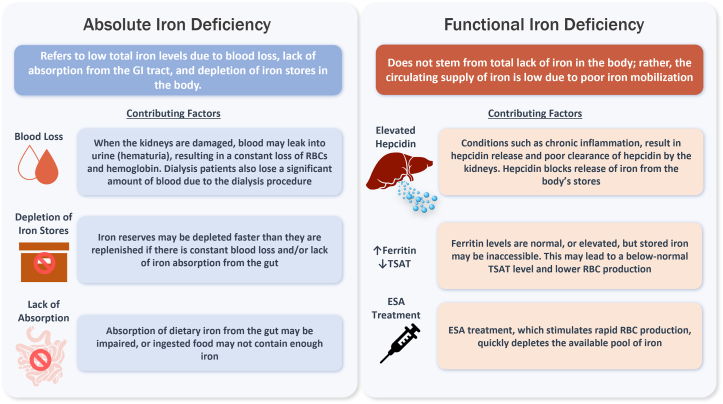
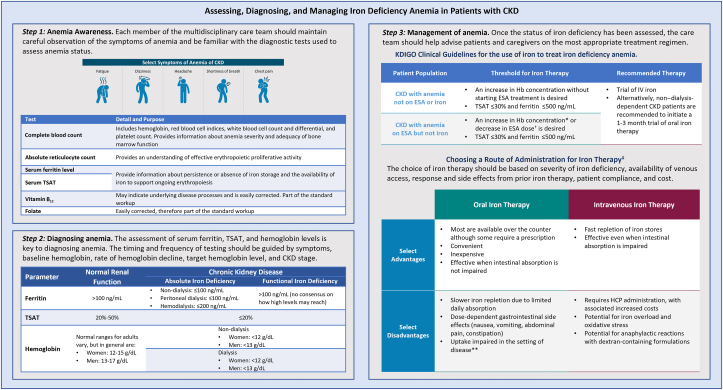
Anemia is a common complication of chronic kidney disease (CKD) and is associated with increased mortality and reduced health-related quality of life. Anemia is characterized by a decrease in hemoglobin, the iron-rich protein that the body uses for oxygen transport. Iron is required to produce hemoglobin, and disruptions in the iron homeostasis can lead to iron-deficiency anemia. Management of anemia in individuals with CKD is typically performed by a team of physicians, nurse practitioners, physician assistants, or registered nurses. Throughout the care continuum, the management can be enhanced by multidisciplinary care, and individuals with CKD can benefit from the involvement of other specialties, with dietitians/nutritionists playing an important role. However, a key area of unmet clinical need is how to assess and address iron-deficiency anemia. This review aims to provide an overview of iron-deficiency anemia in CKD and how this may be diagnosed and managed by the entire kidney care team, such as describing the mechanisms underlying iron homeostasis, the complications of iron-deficiency anemia, and the current challenges associated with its diagnosis and treatment in CKD. Opportunities for each multidisciplinary team member to add value to the care of individuals with CKD and iron-deficiency anemia are also described.
Keywords: Anemia; chronic kidney disease; hemoglobin; iron deficiency; iron metabolism; iron-deficiency anemia.
© 2023 The Authors.
Figures
References
-
- Mariani L., Stengel B., Combe C., et al. The CKD Outcomes and Practice Patterns Study (CKDopps): rationale and methods. Am J Kidney Dis. 2016;68(3):402–413. - PubMed
-
- Thorp M.L., Johnson E.S., Yang X., Petrik A.F., Platt R., Smith D.H. Effect of anaemia on mortality, cardiovascular hospitalizations and end-stage renal disease among patients with chronic kidney disease. Nephrology (Carlton) 2009;14(2):240–246. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
