

Atypical Hemolytic Uremic Syndrome Treated With Ravulizumab or Eculizumab: A Claims-Based Evaluation of Health Care Resource Utilization and Clinical Outcomes in the United States
- PMID: 37415624
- PMCID: PMC10319830
- DOI: 10.1016/j.xkme.2023.100683
Atypical Hemolytic Uremic Syndrome Treated With Ravulizumab or Eculizumab: A Claims-Based Evaluation of Health Care Resource Utilization and Clinical Outcomes in the United States
Abstract
Rationale and objective: Ravulizumab and eculizumab have shown efficacy for the treatment of atypical hemolytic uremic syndrome (aHUS), but real-world evidence for ravulizumab is limited owing to its more recent approval. This real-world database study examined outcomes for adult patients switching to ravulizumab from eculizumab and patients treated with individual treatments.
Study design: A retrospective, observational study using the Clarivate Real World Database.
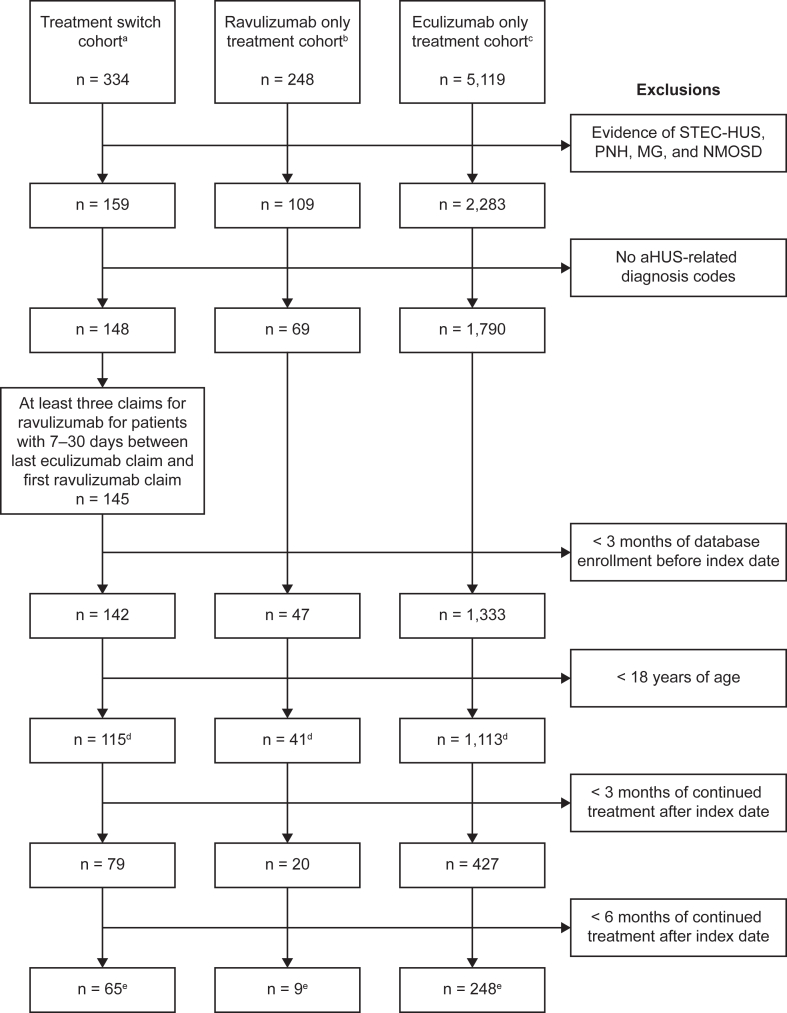
Setting and population: US health-insurance billing data (January 2012 to March 2021) of patients aged 18 years or older with ≥1 diagnosis relevant to aHUS, ≥1 claim for treatment with eculizumab or ravulizumab, and no evidence of other indicated conditions.
Exposures: Treatment-switch (to ravulizumab after eculizumab), ravulizumab-only, and eculizumab-only cohorts were examined.
Outcomes: Clinical procedures, facility visits, health care costs, and clinical manifestations.
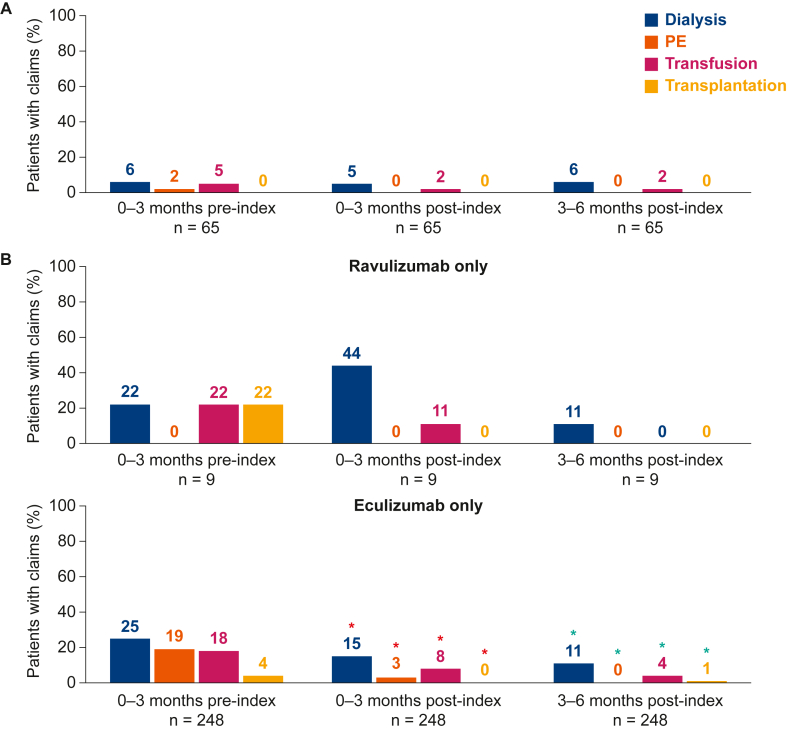
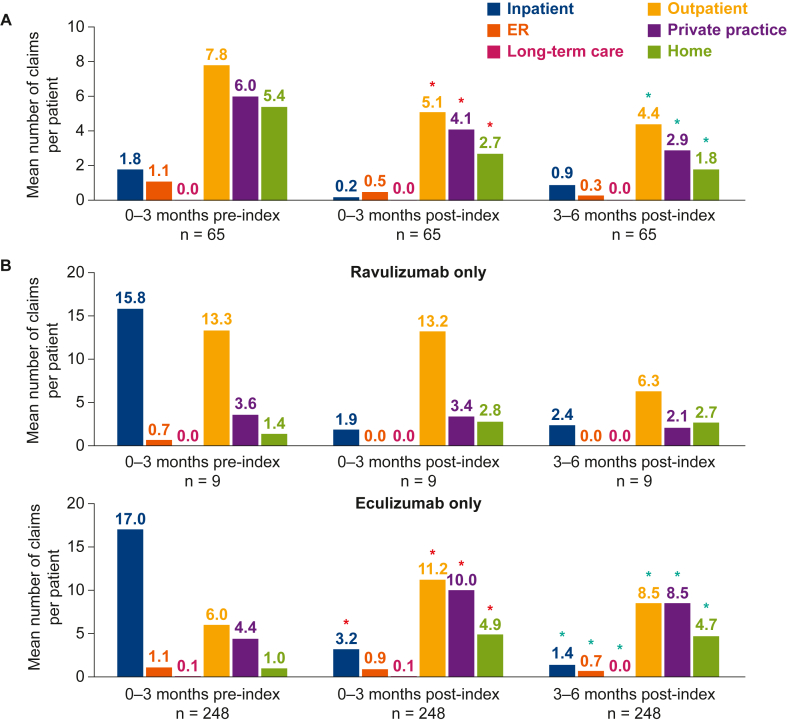
Analytical approach: Paired-sample statistical testing compared the mean numbers of claims for each group 0-3 months before (preindex period) and 0-3 months and 3-6 months after (postindex period) the index date (point of initiation with a single treatment or treatment switch).
Results: In total, 322 patients met the eligibility criteria at 3-6 months postindex in the treatment-switch (n=65), ravulizumab-only (n=9), and eculizumab-only (n=248) cohorts. The proportions of patients with claims for key clinical procedures continued to be small after treatment switch and were small (0%-11%) across all cohorts at 3-6 months postindex. Inpatient visits were reduced in the postindex period across all cohorts. At 3-6 months after treatment switch, patients reported fewer claims for outpatient, private practice, and home visits and lower median health care costs. The proportions of patients with claims for clinical manifestations of aHUS were generally reduced in the postindex period compared with those of the preindex period.
Limitations: Low patient numbers receiving ravulizumab only.
Conclusions: The health-insurance claims data showed a reduced health care burden for US adult patients after treatment with ravulizumab or eculizumab for treatment of aHUS.
Keywords: Complement C5 inhibitors; atypical hemolytic uremic syndrome; outcomes; real-world evidence; treatment patterns.
© 2023 The Authors.
Figures
References
-
- Campistol J.M., Arias M., Ariceta G., et al. An update for atypical haemolytic uraemic syndrome: diagnosis and treatment. A consensus document. Nefrologia. 2015;35(5):421–447. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
