

HIV remission trial investigators' attitudes towards risk and risk mitigation in trials that include treatment interruption
- PMID: 37416088
- PMCID: PMC10319831
- DOI: 10.1016/j.jve.2023.100331
HIV remission trial investigators' attitudes towards risk and risk mitigation in trials that include treatment interruption
Erratum in
-
Corrigendum to "HIV remission trial investigators' attitudes towards risk and risk mitigation in trials that include treatment interruption" [J Virus Erad 9 (2) (June 2023) 100331].J Virus Erad. 2023 Jul 30;9(3):100340. doi: 10.1016/j.jve.2023.100340. eCollection 2023 Sep. J Virus Erad. 2023. PMID: 37560051 Free PMC article.
Abstract
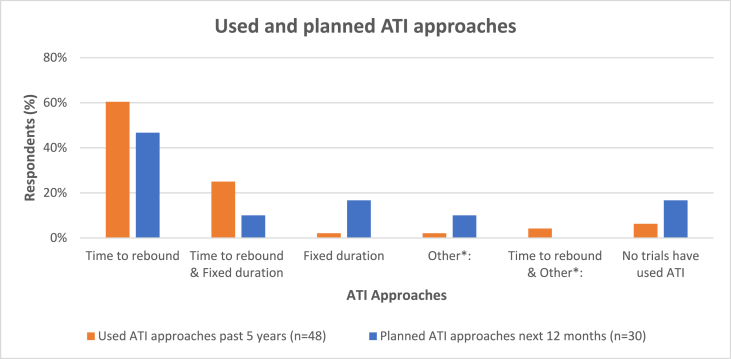
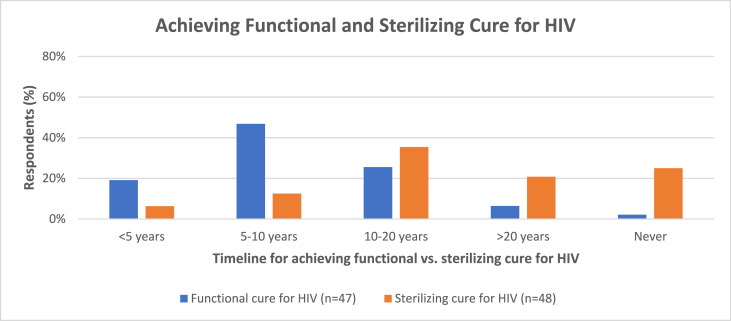
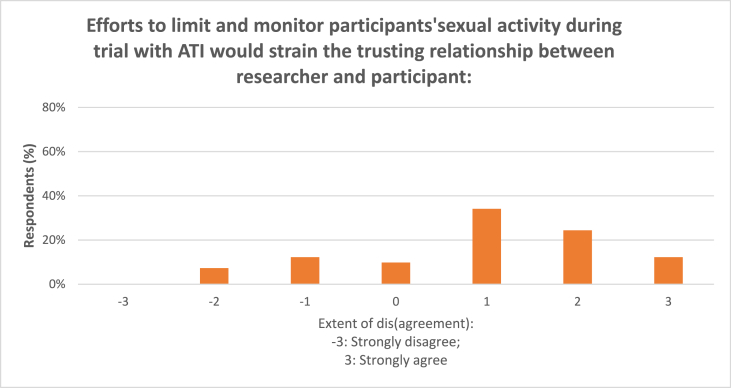
Early-phase HIV remission ("cure") trials aim to test interventions developed to eradicate HIV or to sustainably control HIV without antiretroviral treatment (ART). Many remission trials include analytic treatment interruption (ATI) to evaluate interventions, which increases the risk to participants and their sexual partners. We conducted an online questionnaire of international HIV remission trial investigators and other study team members to assess their expectations regarding the time to achieve long-term control of HIV replication without treatment (functional cure) or complete eradication of replication-competent HIV virus (sterilizing cure); attitudes toward HIV remission research and the feasibility, acceptability, and efficacy of six HIV transmission risk mitigation strategies during trials with ATI of fixed duration. Nearly half of respondents (47%) reported expecting a functional cure for HIV to be achieved in 5-10 years, and one-third (35%) reported 10-20 years for a sterilizing cure to be achieved. On a scale of -3 to 3, mean scores indicated greater respondent concern about the risk of HIV transmission to partners during ATI (Time to rebound Mean: 0.4 and Fixed duration Mean: 11), compared to participant health risks from ATI (Time to Rebound Mean: -.9 and Fixed duration Mean: 0.0). With regard to feasibility, acceptability, and efficacy respectively, mitigation efforts rated positively included: requiring counseling for potential participants (Means: 2.3; 2.1; and 1.1), providing partner referrals for PrEP (Means: 1.3; 1.3; 1.5), providing pre-exposure proxylaxis directly to partners (Means: 1.0; 1.5; 1.6), and monitoring participants for new sexually transmitted disease acquisition (Means: 1.9; 1.4; 1.0). Respondents were less positive about requiring that participants' sexual partner(s) participate in risk counseling or limiting participation to those who commit to abstaining from sex during the entire ATI period. Our study demonstrates that HIV remission trial investigators and study team members are concerned about the risk of transmission to sexual partners during ATI. Separating the assessment of risk mitigation strategies for transmission risk into feasibility, acceptability, and efficacy allows the discovery of strategies that may best achieve all three outcomes. Additional research is needed to compare these more fine-grained assessments with views held by other investigators, people living with HIV, and trial participants.
Keywords: Analytic treatment interruption; Fixed duration; HIV cure; HIV remission Trials; Time to rebound; Transmission to sexual partners.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Dubé K., Kanazawa J., Roebuck C., et al. “We are looking at the future right now”: community acceptability of a home-based viral load test device in the context of HIV cure-related research with analytical treatment interruptions in the United States. HIV Res Clin Pract. 2022 Dec;23(1):120–135. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
