

What is the best reconstruction procedure after esophagectomy? A meta-analysis comparing posterior mediastinal and retrosternal approaches
- PMID: 37416735
- PMCID: PMC10319624
- DOI: 10.1002/ags3.12685
What is the best reconstruction procedure after esophagectomy? A meta-analysis comparing posterior mediastinal and retrosternal approaches
Abstract
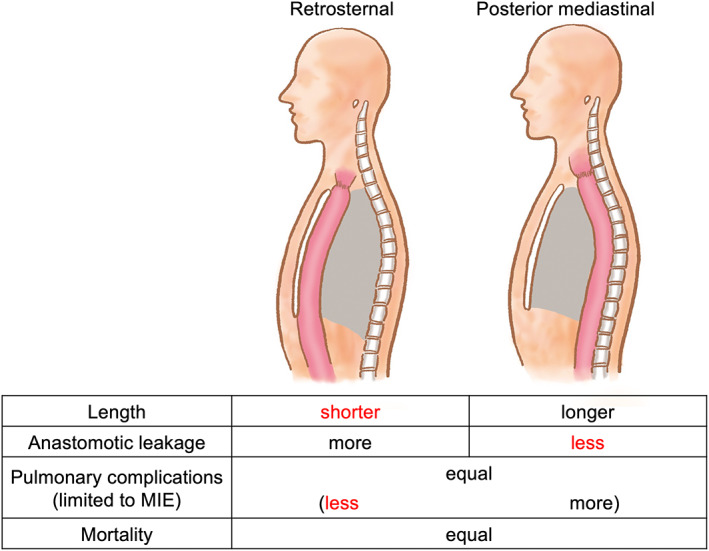
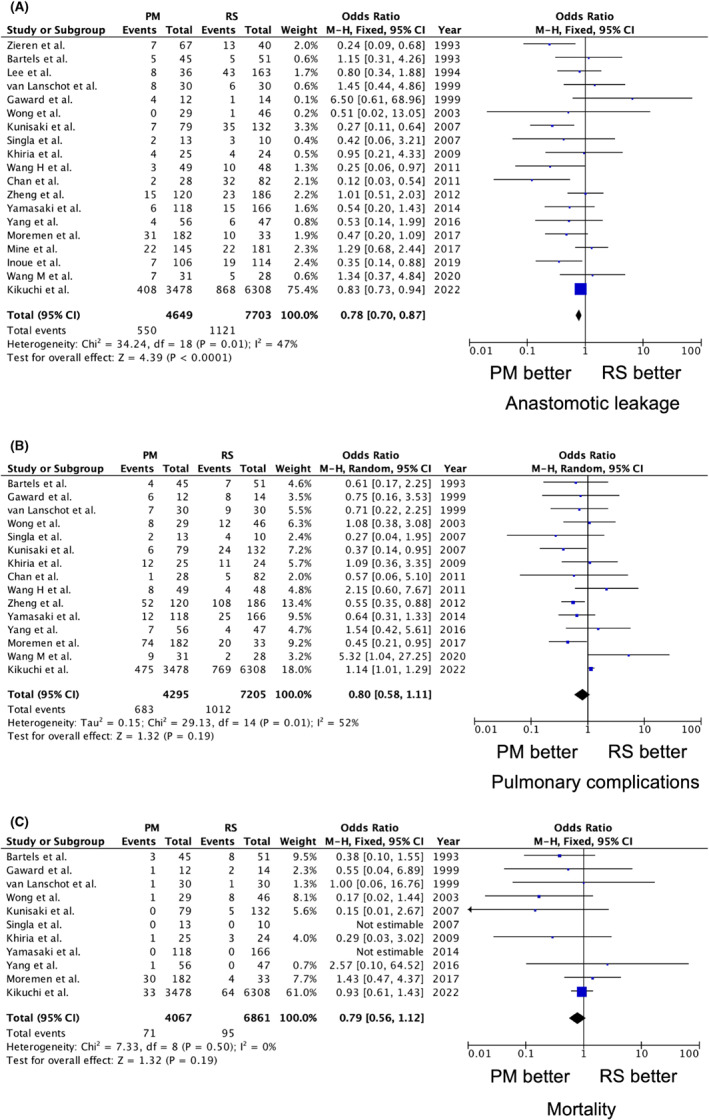
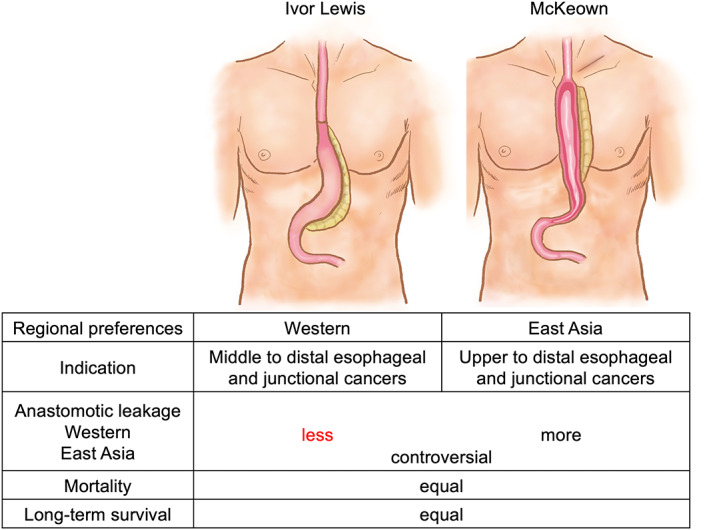
Thoracic esophagectomy is a particularly invasive and complicated surgical procedure, with a reconstruction of the gastrointestinal tract, such as the stomach, jejunum, or colon. The posterior mediastinal, retrosternal, and subcutaneous routes are the three possible esophageal reconstruction routes. Each route has advantages and disadvantages, and the optimal reconstruction route after esophagectomy remains controversial. Additionally, the best anastomotic techniques after esophagectomy in terms of location (Ivor Lewis or McKeown) and suturing (manual or mechanical) are debatable. Our meta-analysis investigating postoperative complications after esophagectomy between the posterior mediastinal and retrosternal routes revealed that the posterior mediastinal route was associated with a significantly lower anastomotic leakage rate than the retrosternal route (odds ratio = 0.78, 95% confidence interval: 0.70-0.87, p < 0.0001). Conversely, pulmonary complications (odds ratio = 0.80, 95% confidence interval: 0.58-1.11, p = 0.19) and mortality between the posterior mediastinal and retrosternal routes (odds ratio = 0.79, 95% confidence interval: 0.56-1.12, p = 0.19) were not significantly different. However, the incidence of pneumonia may be lower when using the retrosternal route rather than the posterior mediastinal route for performing minimally invasive esophagectomy. The McKeown procedure is oncologically necessary for tumors located above the carina to dissect upper mediastinal and cervical lymph nodes; however, the Ivor Lewis procedure offers perioperative and oncological safety for tumors located under the carina. An individualized treatment strategy for selecting the optimal reconstruction procedure can be proposed in future studies based on oncological and patient risk factors considering mid- to long-term quality of life.
Keywords: Ivor Lewis; McKeown; esophageal reconstruction; esophagectomy; posterior mediastinal route; retrosternal route; subcutaneous route.
© 2023 The Authors. Annals of Gastroenterological Surgery published by John Wiley & Sons Australia, Ltd on behalf of The Japanese Society of Gastroenterological Surgery.
Conflict of interest statement
Authors declare no conflict of interests for this article. Hiroya Takeuchi is an editorial board member of Annals of Gastroenterological Surgery.
Figures
Similar articles
-
A comparative study of the lengths of different reconstruction routes used after thoracic esophagectomy.Esophagus. 2021 Jul;18(3):468-474. doi: 10.1007/s10388-020-00805-x. Epub 2021 Jan 19. Esophagus. 2021. PMID: 33462727
-
McKeown or Ivor Lewis totally minimally invasive esophagectomy for cancer of the esophagus and gastroesophageal junction: systematic review and meta-analysis.J Thorac Dis. 2017 Jul;9(Suppl 8):S826-S833. doi: 10.21037/jtd.2017.03.173. J Thorac Dis. 2017. PMID: 28815080 Free PMC article.
-
Anterior versus posterior mediastinal reconstruction after esophagectomy in esophageal cancer patients: a systematic review and meta-analysis.Langenbecks Arch Surg. 2024 Mar 8;409(1):88. doi: 10.1007/s00423-024-03279-y. Langenbecks Arch Surg. 2024. PMID: 38456948
-
[Comparison of retrosternal and posterior mediastinal gastric tube reconstruction after three-phase esophagectomy].Zhonghua Wei Chang Wai Ke Za Zhi. 2010 Jan;13(1):33-5. Zhonghua Wei Chang Wai Ke Za Zhi. 2010. PMID: 20099158 Chinese.
-
Comparison of short-term outcomes between minimally invasive McKeown and Ivor Lewis esophagectomy for esophageal or junctional cancer: a systematic review and meta-analysis.Onco Targets Ther. 2018 Sep 20;11:6057-6069. doi: 10.2147/OTT.S169488. eCollection 2018. Onco Targets Ther. 2018. PMID: 30275710 Free PMC article. Review.
Cited by
-
Current advances and challenges in minimally invasive esophagectomy.Int J Clin Oncol. 2025 Aug;30(8):1463-1474. doi: 10.1007/s10147-025-02806-1. Epub 2025 Jun 19. Int J Clin Oncol. 2025. PMID: 40536623 Review.
-
Long-term follow-up after retrosternal ileocolic esophagoplasty in two cases of long-gap esophageal atresia: why it is still a valid option as a rescue strategy.Front Pediatr. 2023 Nov 22;11:1300802. doi: 10.3389/fped.2023.1300802. eCollection 2023. Front Pediatr. 2023. PMID: 38078333 Free PMC article.
-
A nationwide survey on the safety of cricothyrotomy: a multicenter retrospective study in Japan.Esophagus. 2025 Jan;22(1):19-26. doi: 10.1007/s10388-024-01082-8. Epub 2024 Sep 6. Esophagus. 2025. PMID: 39242403
-
Exploring predictive biomarkers of efficacy and survival with nivolumab treatment for unresectable/recurrent esophageal squamous cell carcinoma.Esophagus. 2025 Jul;22(3):360-372. doi: 10.1007/s10388-025-01120-z. Epub 2025 Apr 24. Esophagus. 2025. PMID: 40274705 Free PMC article.
-
Impact of Dissected Lymph Node Count and Positive Lymph Node Ratio Following Esophagectomy on Long-Term Outcomes in Esophageal Cancer: A Systematic Review and Meta-Analysis.Ann Surg Open. 2025 Jun 13;6(2):e587. doi: 10.1097/AS9.0000000000000587. eCollection 2025 Jun. Ann Surg Open. 2025. PMID: 40557348 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. - PubMed
-
- Booka E, Takeuchi H, Kikuchi H, Hiramatsu Y, Kamiya K, Kawakubo H, et al. Recent advances in thoracoscopic esophagectomy for esophageal cancer. Asian J Endosc Surg. 2019;12(1):19–29. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
