

Postoperative complications and prognosis based on type of surgery in ulcerative colitis patients with colorectal cancer: A multicenter observational study of data from the Japanese Society for Cancer of the Colon and Rectum
- PMID: 37416741
- PMCID: PMC10319604
- DOI: 10.1002/ags3.12659
Postoperative complications and prognosis based on type of surgery in ulcerative colitis patients with colorectal cancer: A multicenter observational study of data from the Japanese Society for Cancer of the Colon and Rectum
Abstract
Background: Patients with ulcerative colitis are reported to be at increased risk of colorectal cancer and are also at high risk of postoperative complications. However, the incidence of postoperative complications in these patients and how the type of surgery performed affects prognosis are not well understood.
Methods: Data collected by the Japanese Society for Cancer of the Colon and Rectum on ulcerative colitis patients with colorectal cancer between January 1983 and December 2020 were analyzed according to whether total colorectal resection was performed with ileoanal anastomosis (IAA), ileoanal canal anastomosis (IACA), or permanent stoma creation. The incidence of postoperative complications and the prognosis for each surgical technique were investigated.
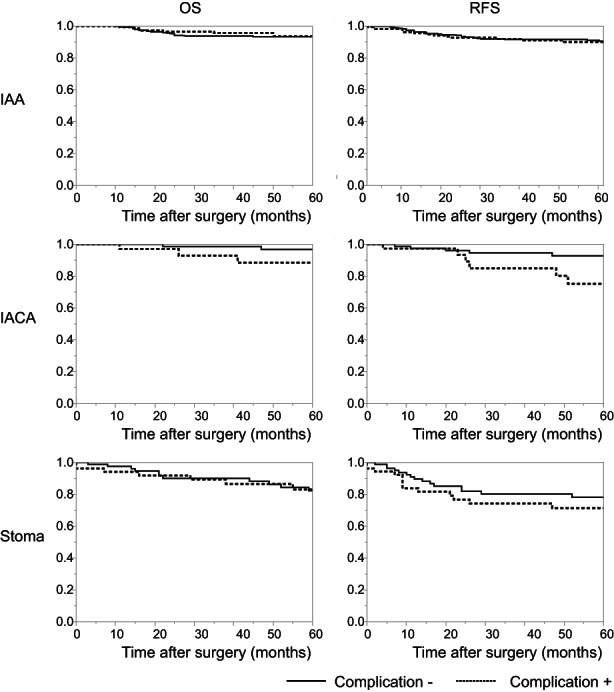
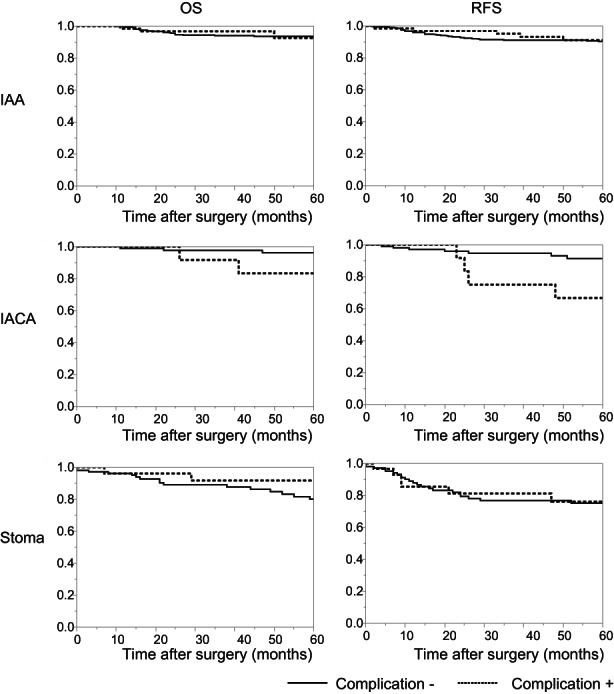
Results: The incidence of overall complications was not significantly different among the IAA, IACA, and stoma groups (32.7%, 32.3%, and 37.7%, respectively; p = 0.510). The incidence of infectious complications was significantly higher in the stoma group (21.2%) than in the IAA (12.9%) and IACA (14.6%) groups (p = 0.048); however, the noninfectious complication rate was lower in the stoma group (13.7%) than in the IAA (21.1%) and IACA (16.2%) groups (p = 0.088). Five-year relapse-free survival was higher in patients without complications than in those with complications in the IACA group (92.8% vs. 75.2%; p = 0.041) and the stoma group (78.1% vs. 71.2%, p = 0.333) but not in the IAA group (90.3% vs. 90.0%, p = 0.888).
Conclusion: The risks of infectious and noninfectious complications differed according to the type of surgical technique used. Postoperative complications worsened prognosis.
Keywords: colorectal neoplasms; postoperative complication; prognosis; ulcerative colitis.
© 2023 The Authors. Annals of Gastroenterological Surgery published by John Wiley & Sons Australia, Ltd on behalf of The Japanese Society of Gastroenterological Surgery.
Conflict of interest statement
The authors declare no conflicts of interest for this article.
Figures


Similar articles
-
Ileoanal anastomosis for ulcerative colitis: results of an evolutionary surgical procedure.Hepatogastroenterology. 1998 Nov-Dec;45(24):2123-6. Hepatogastroenterology. 1998. PMID: 9951877
-
[Differential indications for ileoanal pouch anastomosis : Ulcerative colitis, familial adenomatous polyposis, synchronous colorectal cancer - Crohn's disease, constipation].Chirurg. 2017 Jul;88(7):555-558. doi: 10.1007/s00104-017-0421-4. Chirurg. 2017. PMID: 28405717 Review. German.
-
[Surgical Treatment Outcome of Patients with Colorectal Cancer Having Ulcerative Colitis].Gan To Kagaku Ryoho. 2018 Dec;45(13):2054-2056. Gan To Kagaku Ryoho. 2018. PMID: 30692282 Japanese.
-
Surgical complications in relation to functional outcomes after ileoanal anastomosis in pediatric patients with ulcerative colitis.J Pediatr Surg. 2007 Feb;42(2):290-5. doi: 10.1016/j.jpedsurg.2006.10.001. J Pediatr Surg. 2007. PMID: 17270537
-
Perianal Fistula After Ileoanal Pouch in Patients With Ulcerative Colitis: A Review of 475 Patients Operated on at a Major IBD Center.Dis Colon Rectum. 2022 Jan 1;65(1):76-82. doi: 10.1097/DCR.0000000000002114. Dis Colon Rectum. 2022. PMID: 34882630 Review.
References
-
- Ananthakrishnan AN, Kaplan GG, Bernstein CN, Burke KE, Lochhead PJ, Sasson AN, et al. Lifestyle, behaviour, and environmental modification for the management of patients with inflammatory bowel diseases: an International Organization for Study of inflammatory bowel diseases consensus. Lancet Gastroenterol Hepatol. 2022;7:666–78. - PubMed
-
- Bohl JL, Sobba K. Indications and options for surgery in ulcerative colitis. Surg Clin North Am. 2015;95:1211–32. - PubMed
