

Clinical outcomes and predictors of success with Impella weaning in cardiogenic shock: a single-center experience
- PMID: 37416919
- PMCID: PMC10321515
- DOI: 10.3389/fcvm.2023.1171956
Clinical outcomes and predictors of success with Impella weaning in cardiogenic shock: a single-center experience
Abstract
Introduction: Cardiogenic shock (CS) is a severe syndrome with poor prognosis. Short-term mechanical circulatory support with Impella devices has emerged as an increasingly therapeutic option, unloading the failing left ventricle (LV) and improving hemodynamic status of affected patients. Impella devices should be used for the shortest time necessary to allow LV recovery because of time-dependent device-related adverse events. The weaning from Impella, however, is mostly performed in the absence of established guidelines, mainly based on the experience of the individual centres.
Methods: The aim of this single center study was to retrospectively evaluate whether a multiparametrical assessment before and during Impella weaning could predict successful weaning. The primary study outcome was death occurring during Impella weaning and secondary endpoints included assessment of in-hospital outcomes.
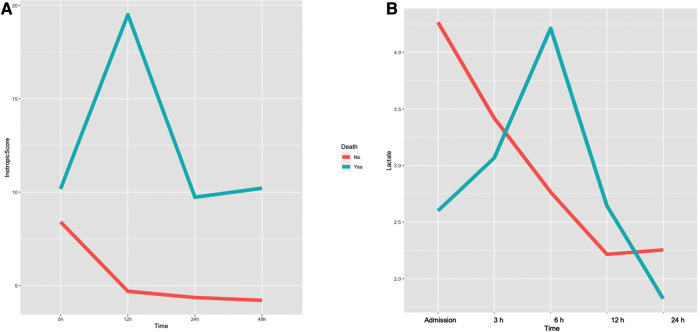
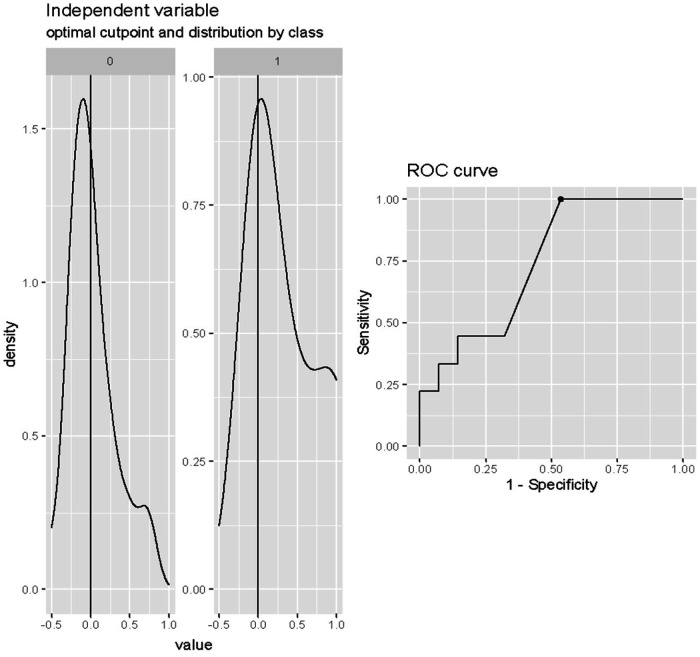
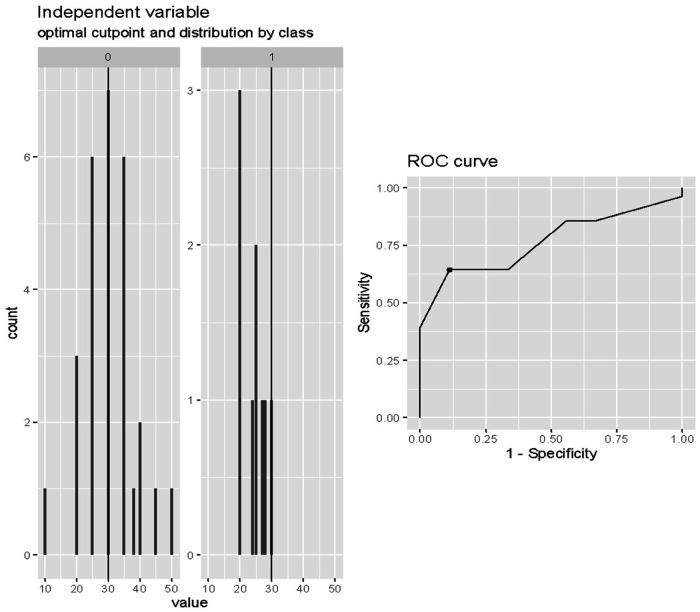
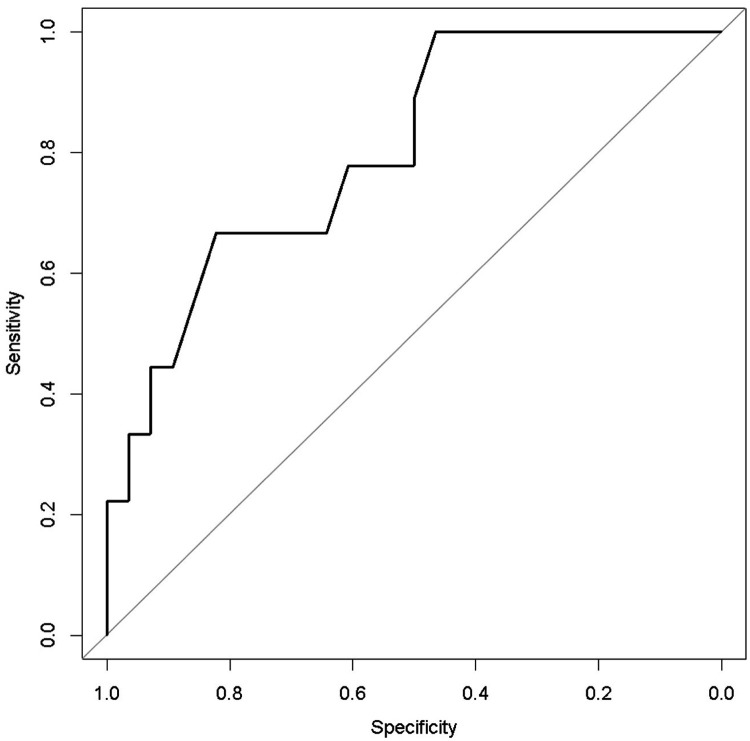
Results: Of a total of 45 patients (median age, 60 [51-66] years, 73% male) treated with an Impella device, 37 patients underwent impella weaning/removal and 9 patients (20%) died after the weaning. Non-survivors patients after impella weaning more commonly had a previous history of known heart failure (p = 0.054) and an implanted ICD-CRT (p = 0.01), and were more frequently treated with continuous renal replacement therapy (p = 0.02). In univariable logistic regression analysis, lactates variation (%) during the first 12-24 h of weaning, lactate value after 24 h of weaning, left ventricular ejection fraction (LVEF) at the beginning of weaning, and inotropic score after 24 h from weaning beginning were associated with death. Stepwise multivariable logistic regression identified LVEF at the beginning of weaning and lactates variation (%) in the first 12-24 h from weaning beginning as the most accurate predictors of death after weaning. The ROC analysis indicated 80% accuracy (95% confidence interval = 64%-96%) using the two variables in combination to predict death after weaning from Impella.
Conclusions: This single-center experience on Impella weaning in CS showed that two easily accessible parameters as LVEF at the beginning of weaning and lactates variation (%) in the first 12-24 h from weaning begin were the most accurate predictors of death after weaning.
Keywords: Impella; cardiogenic shock; complications; heart failure; outcomes; weaning.
© 2023 Matassini, Marini, Angelozzi, Angelini, Shkoza, Compagnucci, Falanga, Battistoni, Pongetti, Francioni, Piva, Mucaj, Nicolini, Maolo, Di Eusanio, Munch, Dello Russo and Perna.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin ML, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. (2022) 79(17):e263–421. 10.1016/j.jacc.2021.12.012 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials