2022 Seoul Consensus on Clinical Practice Guidelines for Functional Constipation
- PMID: 37417257
- PMCID: PMC10334201
- DOI: 10.5056/jnm23066
2022 Seoul Consensus on Clinical Practice Guidelines for Functional Constipation
Abstract
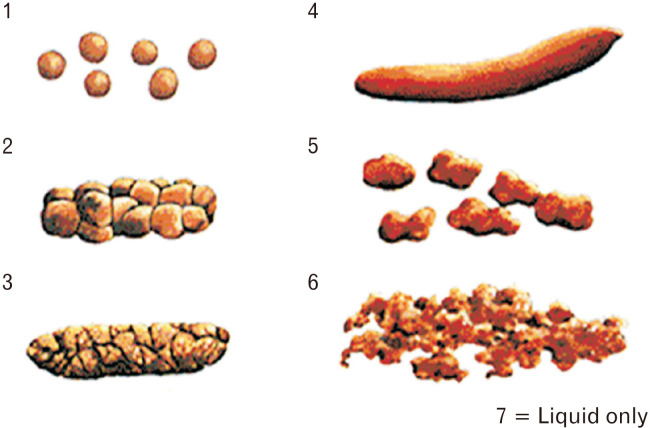
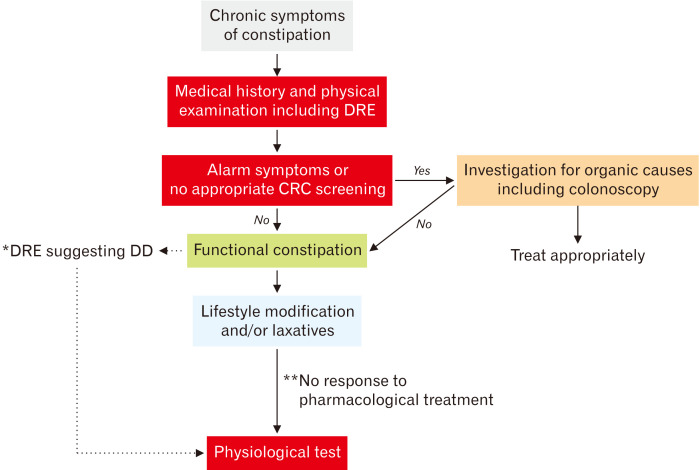
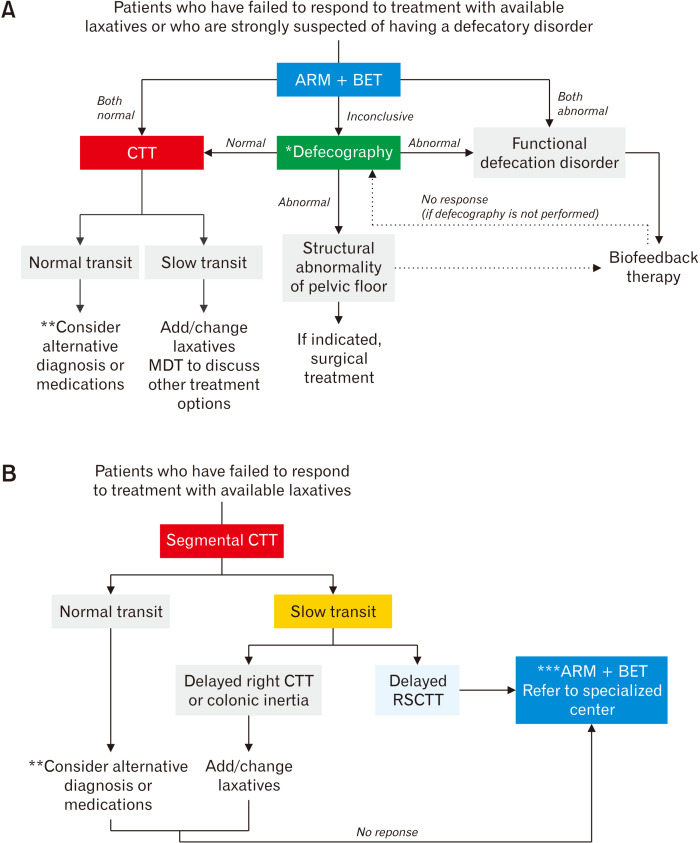
Chronic constipation is one of the most common digestive diseases encountered in clinical practice. Constipation manifests as a variety of symptoms, such as infrequent bowel movements, hard stools, feeling of incomplete evacuation, straining at defecation, a sense of anorectal blockage during defecation, and use of digital maneuvers to assist defecation. During the diagnosis of chronic constipation, the Bristol Stool Form Scale, colonoscopy, and a digital rectal examination are useful for objective symptom evaluation and differential diagnosis of secondary constipation. Physiological tests for functional constipation have complementary roles and are recommended for patients who have failed to respond to treatment with available laxatives and those who are strongly suspected of having a defecatory disorder. As new evidence on the diagnosis and management of functional constipation emerged, the need to revise the previous guideline was suggested. Therefore, these evidence-based guidelines have proposed recommendations developed using a systematic review and meta-analysis of the treatment options available for functional constipation. The benefits and cautions of new pharmacological agents (such as lubiprostone and linaclotide) and conventional laxatives have been described through a meta-analysis. The guidelines consist of 34 recommendations, including 3 concerning the definition and epidemiology of functional constipation, 9 regarding diagnoses, and 22 regarding managements. Clinicians (including primary physicians, general health professionals, medical students, residents, and other healthcare professionals) and patients can refer to these guidelines to make informed decisions regarding the management of functional constipation.
Keywords: Constipation; Diagnosis; Guideline; Meta-analysis; Therapeutics.
Conflict of interest statement
Figures
Similar articles
-
[Seoul Consensus on Clinical Practice Guidelines for Functional Constipation].Korean J Gastroenterol. 2025 Jul 25;85(3):319-344. doi: 10.4166/kjg.2024.156. Korean J Gastroenterol. 2025. PMID: 40709424 Korean.
-
[Diagnosis of Chronic Constipation].Korean J Gastroenterol. 2024 May 25;83(5):179-183. doi: 10.4166/kjg.2024.039. Korean J Gastroenterol. 2024. PMID: 38783618 Review. Korean.
-
Constipation: Pathophysiology and Current Therapeutic Approaches.Handb Exp Pharmacol. 2017;239:59-74. doi: 10.1007/164_2016_111. Handb Exp Pharmacol. 2017. PMID: 28185025 Review.
-
Symptoms in chronic constipation.Dis Colon Rectum. 1997 Aug;40(8):902-6. doi: 10.1007/BF02051196. Dis Colon Rectum. 1997. PMID: 9269805
-
Clinical Practice Guideline: Irritable bowel syndrome with constipation and functional constipation in the adult.Rev Esp Enferm Dig. 2016 Jun;108(6):332-63. doi: 10.17235/reed.2016.4389/2016. Rev Esp Enferm Dig. 2016. PMID: 27230827 Review.
Cited by
-
Clinical Yield of Colonoscopy in Evaluation of Young Women with Constipation: An Age- and Gender-Based Analysis.Diagnostics (Basel). 2025 May 11;15(10):1209. doi: 10.3390/diagnostics15101209. Diagnostics (Basel). 2025. PMID: 40428202 Free PMC article.
-
Diet, Physical Activity, and Chronic Constipation: Unveiling the Combined Effects for Better Treatment Strategies.J Neurogastroenterol Motil. 2024 Jul 30;30(3):255-256. doi: 10.5056/jnm24085. J Neurogastroenterol Motil. 2024. PMID: 38972861 Free PMC article. No abstract available.
-
A randomized, double-blind, placebo-controlled clinical study to evaluate the efficacy and safety of Weizmannia coagulans BC99 in the treatment of chronic constipation in adults.Front Nutr. 2024 Jul 25;11:1395083. doi: 10.3389/fnut.2024.1395083. eCollection 2024. Front Nutr. 2024. PMID: 39119466 Free PMC article.
-
Constipation and colonoscopy.World J Gastrointest Endosc. 2024 May 16;16(5):244-249. doi: 10.4253/wjge.v16.i5.244. World J Gastrointest Endosc. 2024. PMID: 38813573 Free PMC article.
-
Efficacy and mechanism of acupuncture for functional constipation in older adults: study protocol for a randomized controlled trial.Front Neurol. 2024 Apr 15;15:1341861. doi: 10.3389/fneur.2024.1341861. eCollection 2024. Front Neurol. 2024. PMID: 38685950 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials