

A novel de-escalation antiplatelet therapy for patients with acute coronary syndrome undergoing percutaneous coronary intervention
- PMID: 37417626
- PMCID: PMC10328641
- DOI: 10.1097/MD.0000000000034153
A novel de-escalation antiplatelet therapy for patients with acute coronary syndrome undergoing percutaneous coronary intervention
Abstract
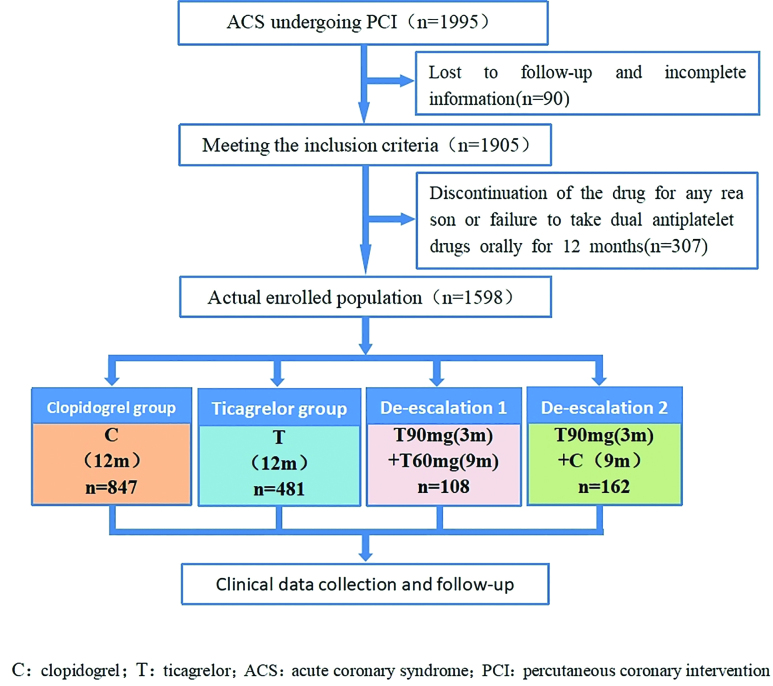
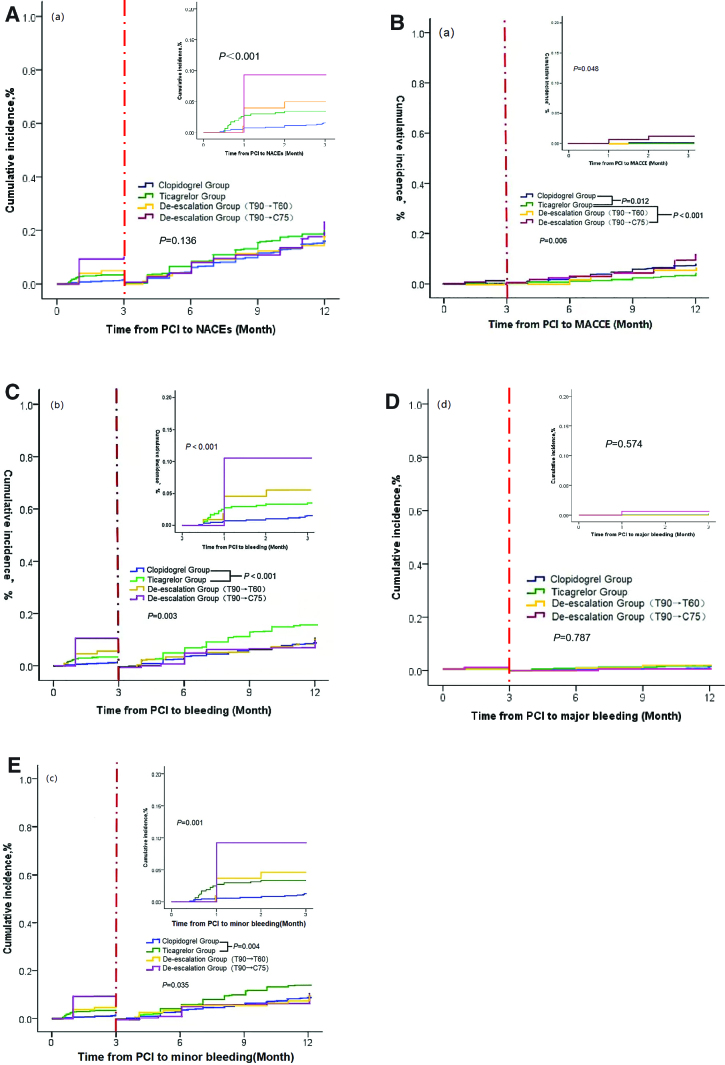
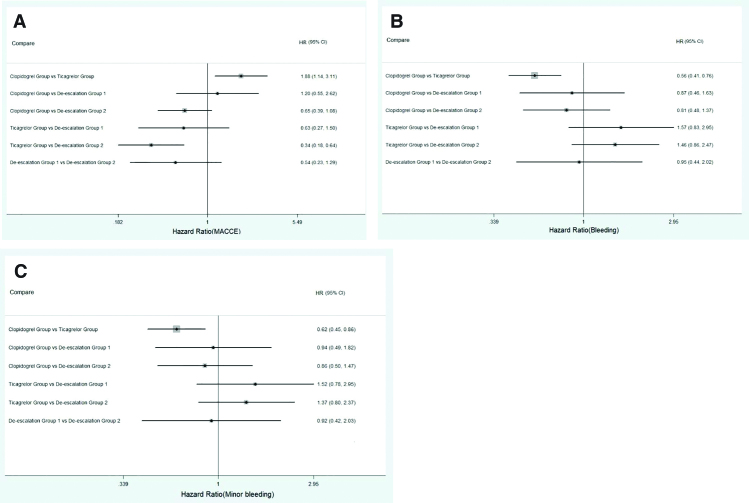
To investigate the effect of different DAPTs in patients with ACS undergoing PCI, and to identify the most efficient DAPT to reduce the risk of ischemia and bleeding after PCI. Between March 2017 and December 2021, 1598 patients with ACS who underwent PCI were included in the study. The DAPT protocol included the clopidogrel group (aspirin 100 mg + clopidogrel 75 mg), ticagrelor group (aspirin 100 mg + ticagrelor 90 mg), de-escalation Group 1 (reduced dose of ticagrelor [from 90 mg to 60 mg]) after 3 months of oral DAPT [aspirin 100 mg + ticagrelor 90 mg]), and de-escalation Group 2 (switched from ticagrelor to clopidogrel after 3 months of oral DAPT [aspirin 100 mg + ticagrelor 90 mg]). All patients received a 12-month follow-up. The primary endpoint was net adverse clinical events (NACEs) that included the composite endpoints of cardiac death, myocardial infarction, ischemia-driven revascularization, stroke, and bleeding events. There were 2 secondary endpoints, major adverse cardiovascular and cerebrovascular events (MACCEs) and bleeding. No statistically significant difference was found in the incidence of NACEs between the 4 groups at the average 12-month follow-up (15.7% vs 19.2% vs 16.7% vs 20.4%). Cox regression analysis revealed that DAPT ticagrelor group regimen (hazard ratio [HR] 0.547; 95% confidence interval [CI]: 0.334-0.896; P = .017) were associated with a lower risk of MACCEs. Age (HR 1.024; 95% CI: 1.003-1.046; P = .022). DAPT de-escalation Group 2 regimen (HR 1.665; 95% CI: 1.001-2.767; P = .049) were marginally associated with a higher risk of MACCEs. Ticagrelor group regimen (HR 1.856; 95% CI: 1.376-2.504; P < .001) was associated with higher risk of bleeding events. Ticagrelor group regimen (HR 1.606; 95% CI: 1.179-2.187; P = .003) were associated with a higher risk of minor bleeding events. For patients with ACS underwent PCI, there were no significant difference in the incidence of NACEs between 3 and 12 months after PCI between de-escalation and non-de-escalation therapies. Compared with ticagrelor-based 12-month DAPT, there was no significant difference in MACCEs and bleeding events in patients receiving de-escalation treatment (ticagrelor reduction from 90 to 60 mg, 3 months after PCI).
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Effectiveness of dual antiplatelet de-escalation therapy on the prognosis of patients with ST segment elevation myocardial infarction undergoing percutaneous coronary intervention.BMC Cardiovasc Disord. 2023 Mar 29;23(1):168. doi: 10.1186/s12872-023-03152-8. BMC Cardiovasc Disord. 2023. PMID: 36991321 Free PMC article.
-
Unguided de-escalation from ticagrelor to clopidogrel in stabilised patients with acute myocardial infarction undergoing percutaneous coronary intervention (TALOS-AMI): an investigator-initiated, open-label, multicentre, non-inferiority, randomised trial.Lancet. 2021 Oct 9;398(10308):1305-1316. doi: 10.1016/S0140-6736(21)01445-8. Lancet. 2021. PMID: 34627490 Clinical Trial.
-
Comparison of one-month versus twelve-month dual antiplatelet therapy after implantation of drug-eluting stents guided by either intravascular ultrasound or angiography in patients with acute coronary syndrome: rationale and design of prospective, multicenter, randomized, controlled IVUS-ACS and ULTIMATE-DAPT trial.Am Heart J. 2021 Jun;236:49-58. doi: 10.1016/j.ahj.2021.02.014. Epub 2021 Feb 20. Am Heart J. 2021. PMID: 33621541
-
Safety and Efficacy of Ticagrelor versus Clopidogrel in East Asian Patients with Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention Treated with Dual Antiplatelet Therapy: A Meta-Analysis of Randomized Controlled Trials.Cardiology. 2023;148(4):363-373. doi: 10.1159/000530602. Epub 2023 Apr 24. Cardiology. 2023. PMID: 37094558 Free PMC article.
-
De-escalation from Prasugrel or Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome Managed with Percutaneous Coronary Intervention: An Updated Meta-analysis of Randomized Clinical Trials.Am J Cardiovasc Drugs. 2022 May;22(3):287-298. doi: 10.1007/s40256-021-00504-7. Epub 2021 Oct 15. Am J Cardiovasc Drugs. 2022. PMID: 34651261
Cited by
-
EValuation of Acute and Early Phase P2Y12 Inhibitor DE-escalation After PerCutaneous Intervention (EVADE PCI).Kans J Med. 2025 Apr 14;18(2):31-34. doi: 10.17161/kjm.vol18.22921. eCollection 2025 Mar-Apr. Kans J Med. 2025. PMID: 40476260 Free PMC article.
References
-
- Valgimigli M, Bueno H, Byrne RA, et al. .; ESC Scientific Document Group. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the task force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018;39:213–60. - PubMed
-
- Ibanez B, James S, Agewall S, et al. .; ESC Scientific Document Group. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–77. - PubMed
-
- Neumann FJ, Sousa-Uva M, Ahlsson A, et al. .; ESC Scientific Document Group. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165. - PubMed
-
- Collet JP, Thiele H, Barbato E, et al. .; ESC Scientific Document Group. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42:1289–367. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
