

Multiaxial pressure-strain analysis of regional myocardial work in the setting of graded coronary stenoses and dobutamine stress
- PMID: 37417870
- PMCID: PMC10538990
- DOI: 10.1152/ajpheart.00735.2022
Multiaxial pressure-strain analysis of regional myocardial work in the setting of graded coronary stenoses and dobutamine stress
Abstract
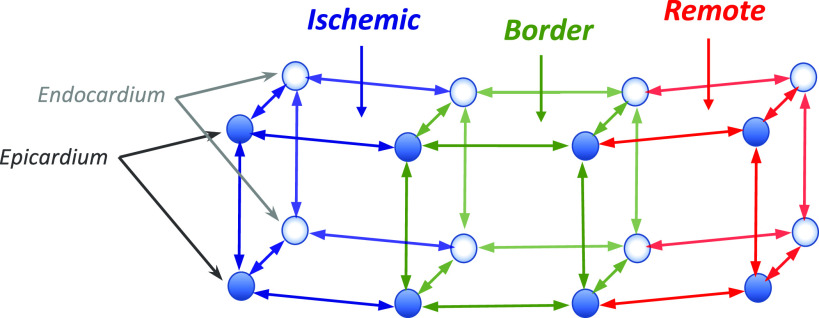
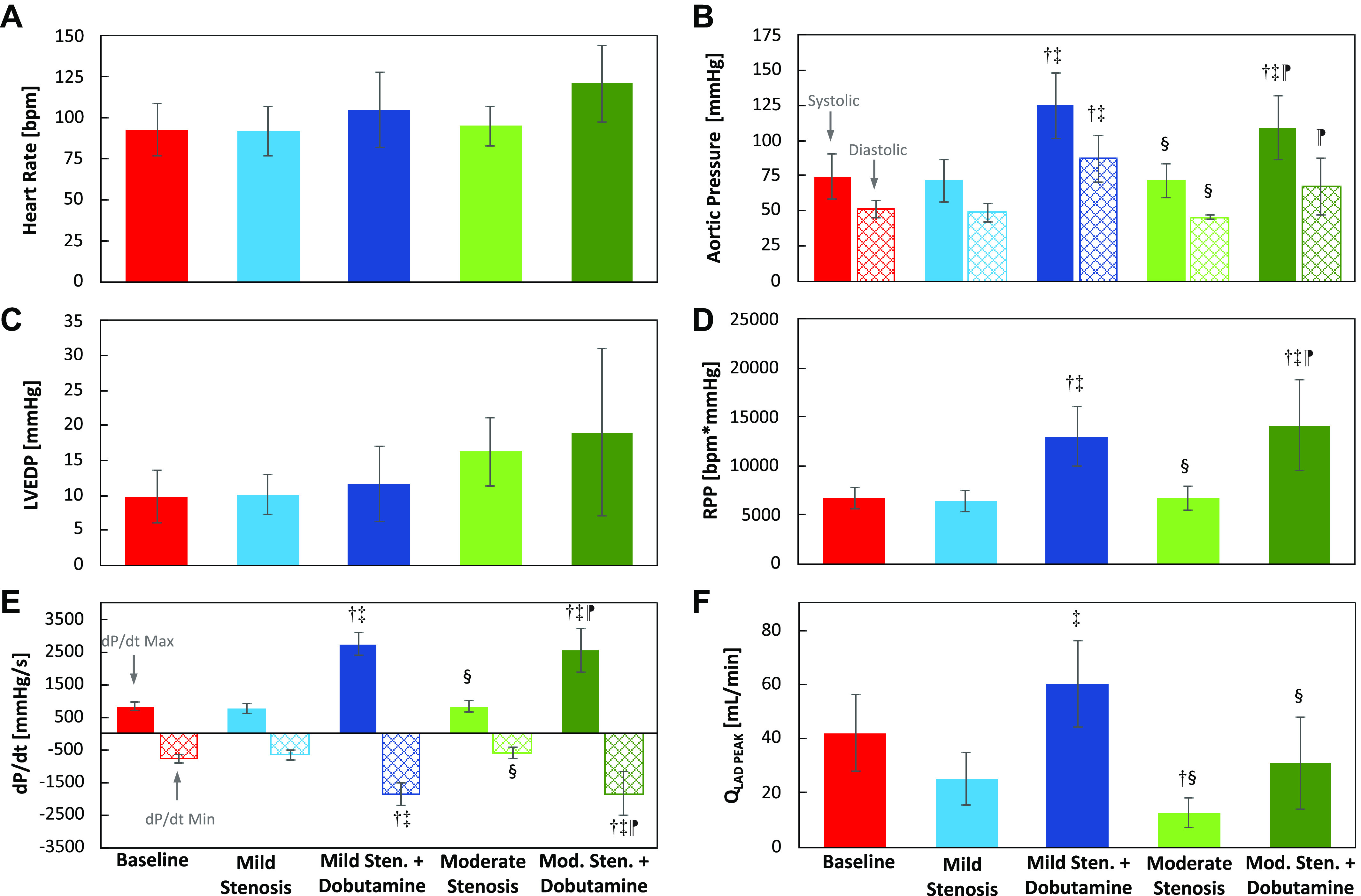
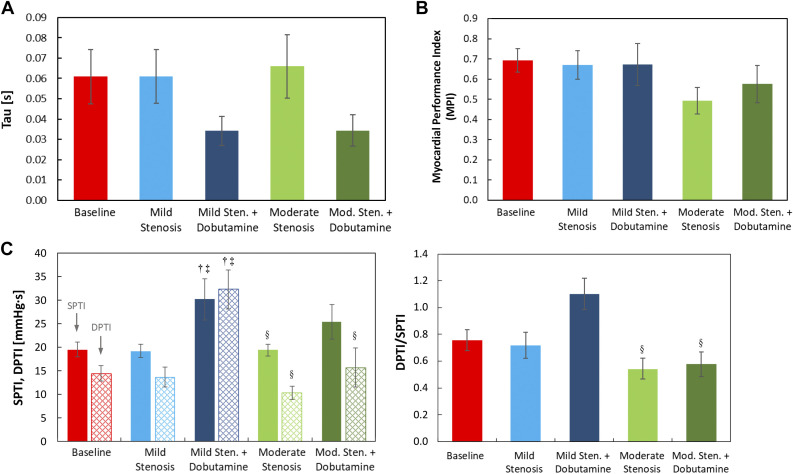
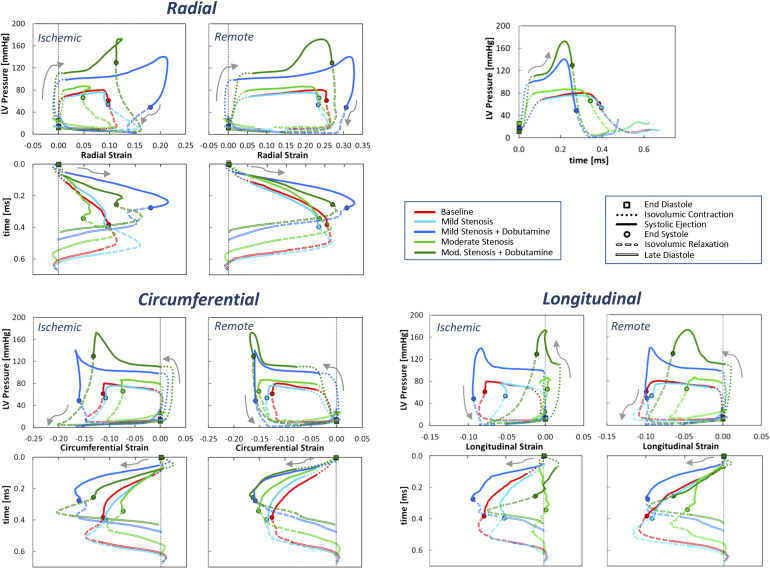
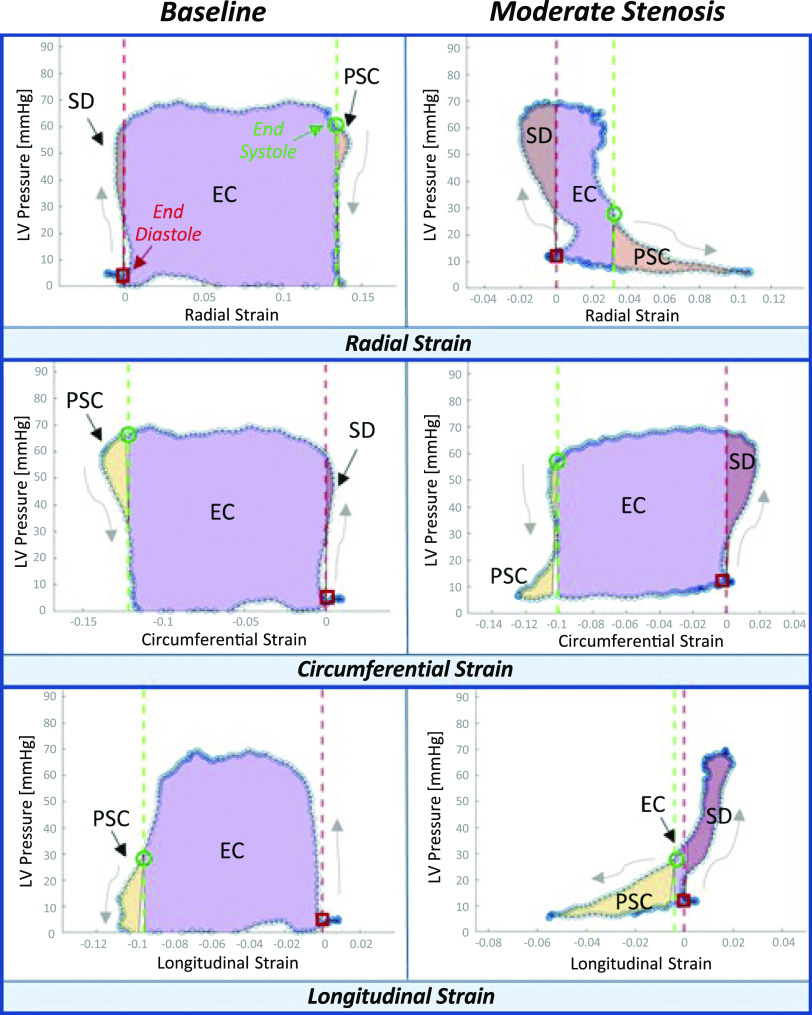
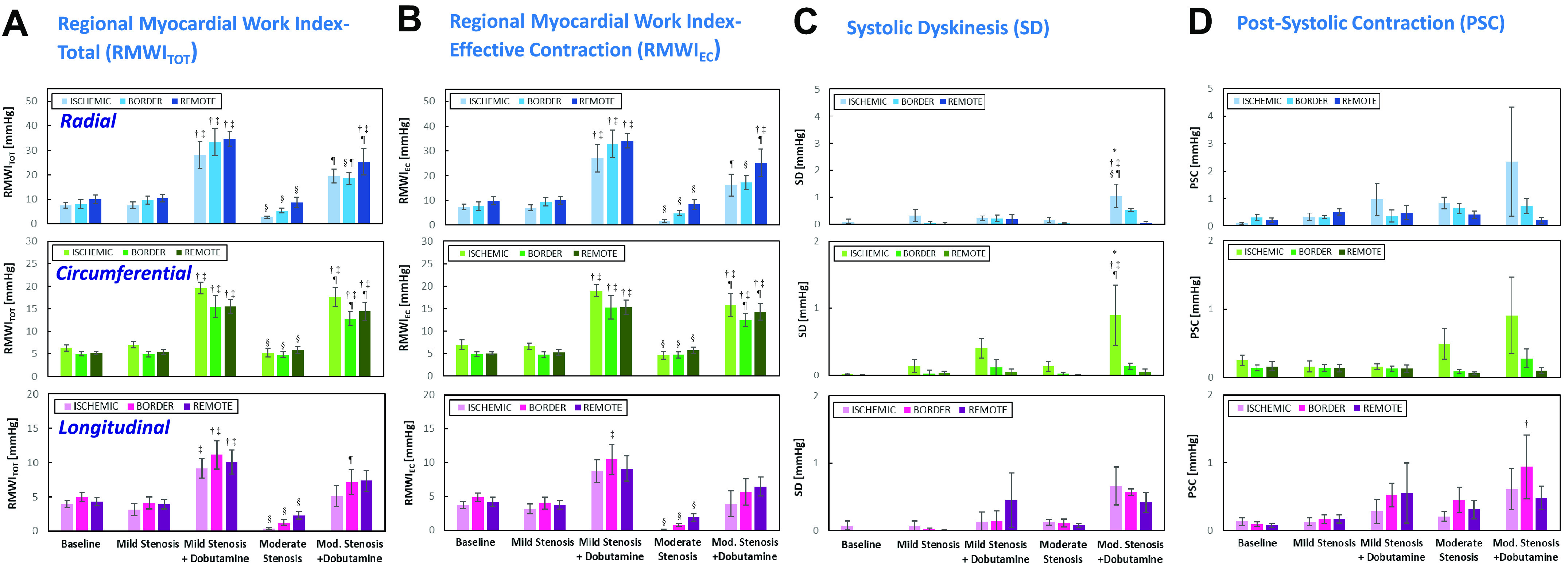
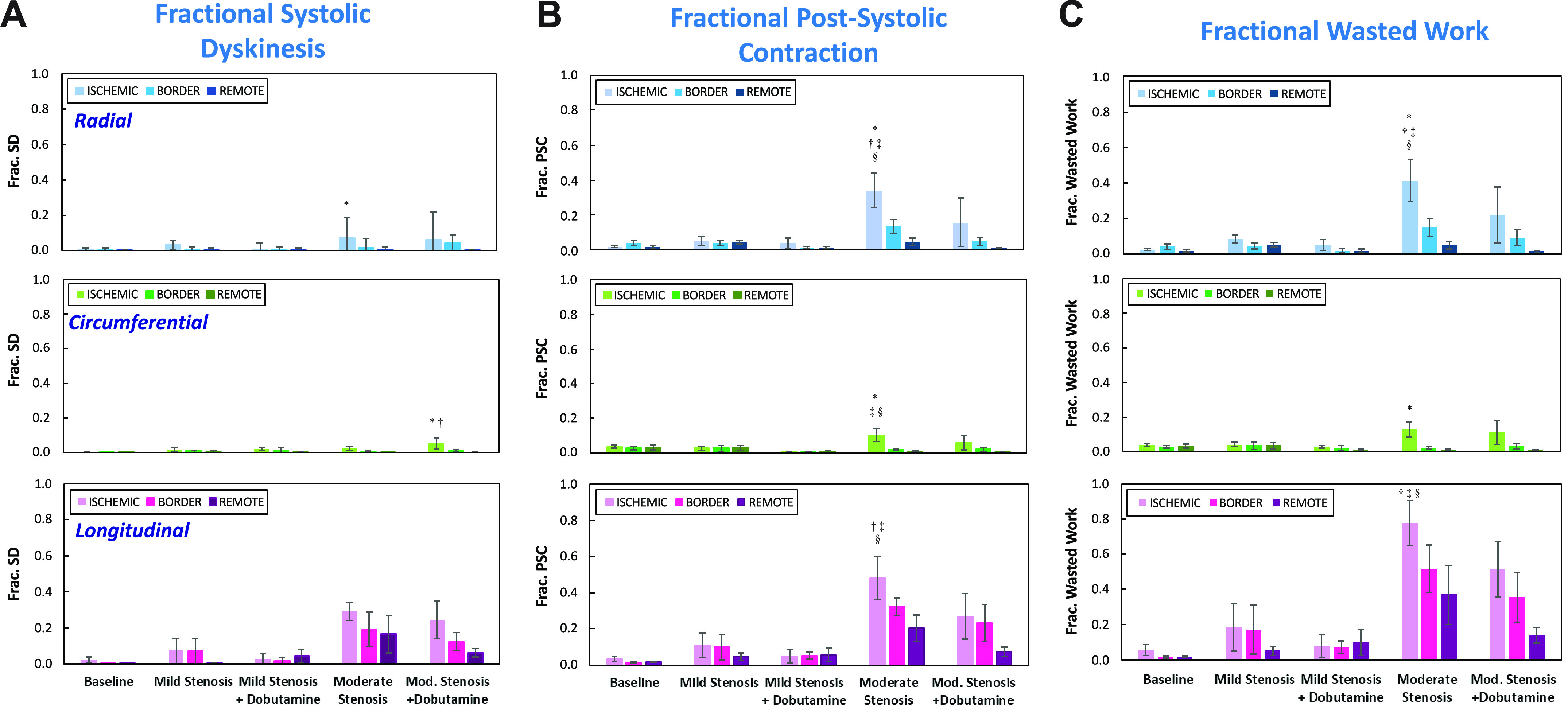
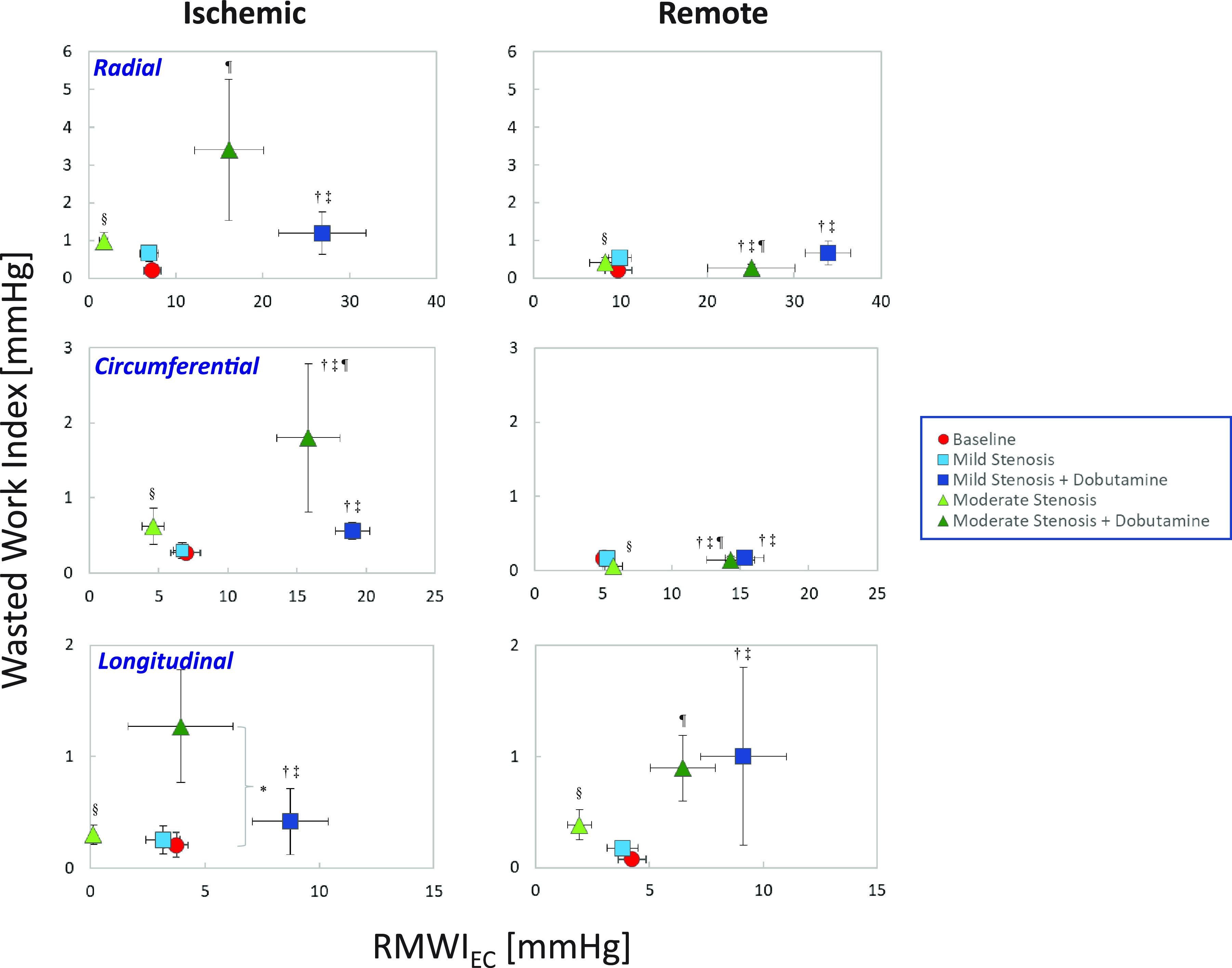
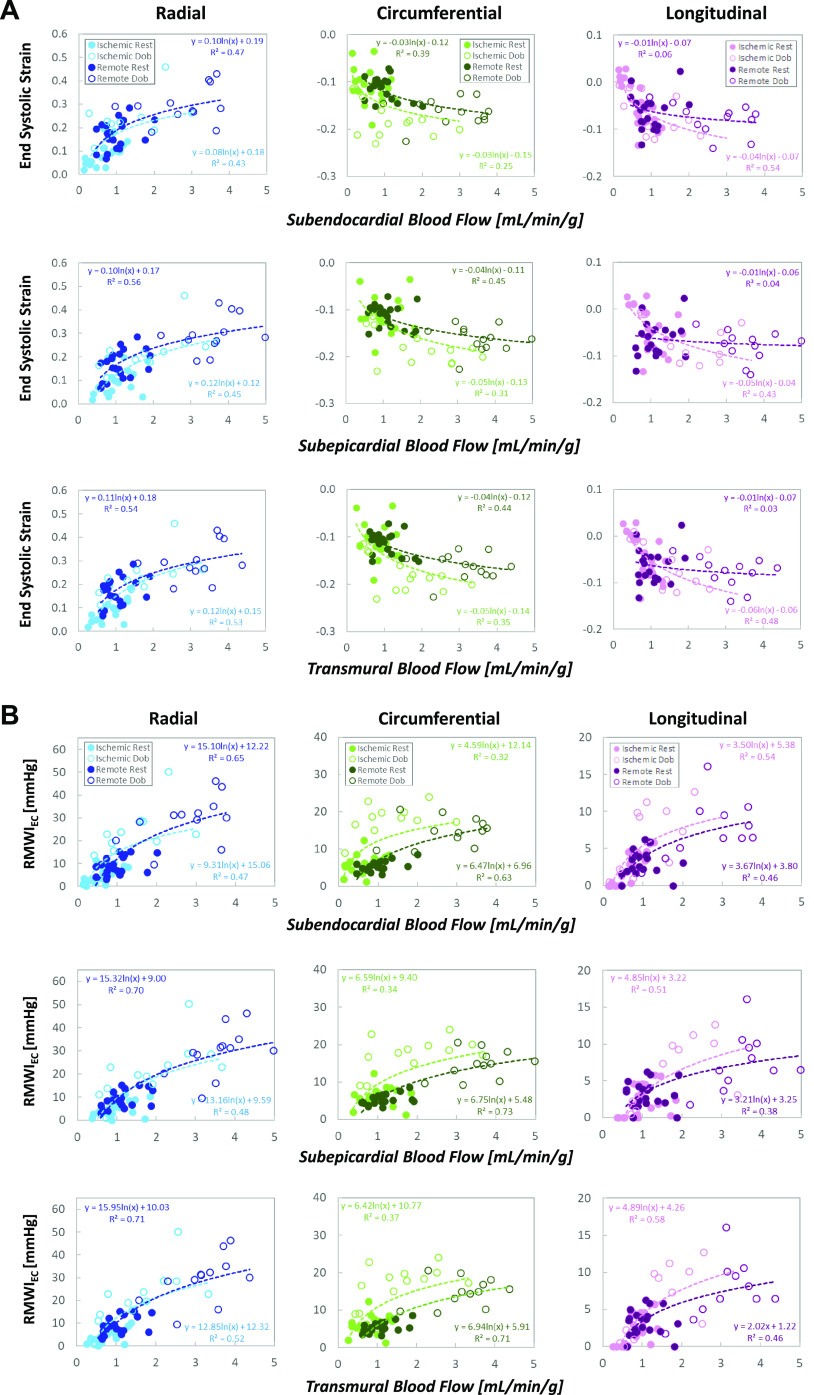
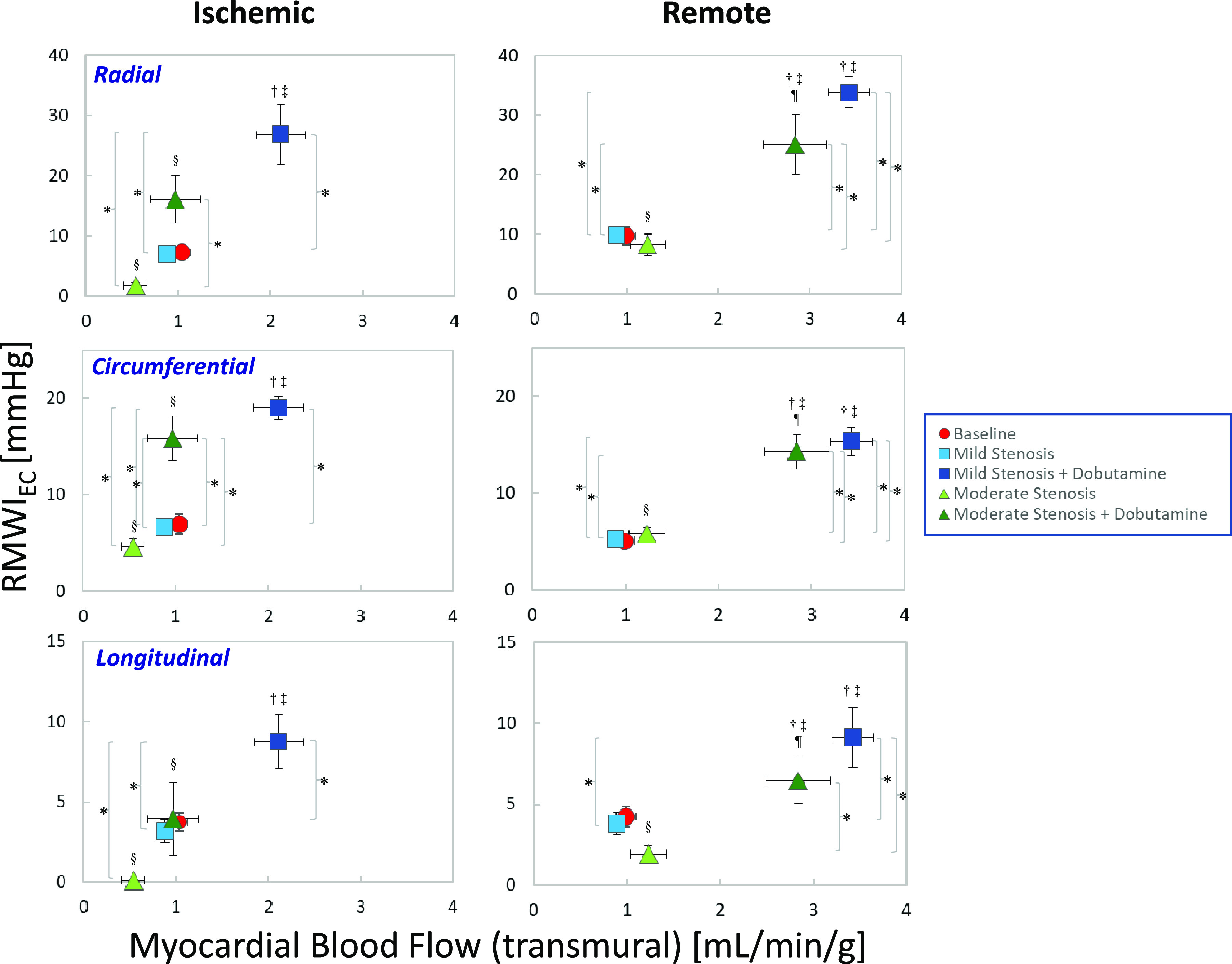
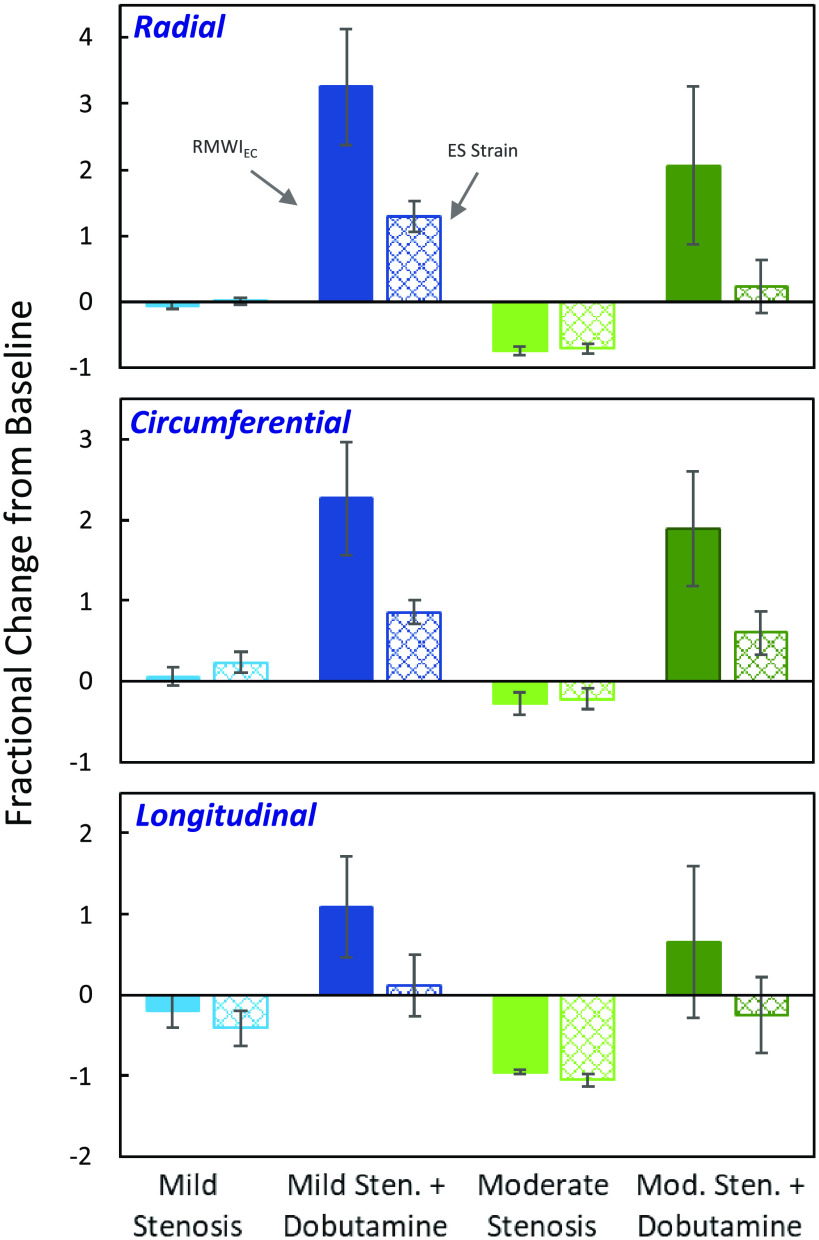
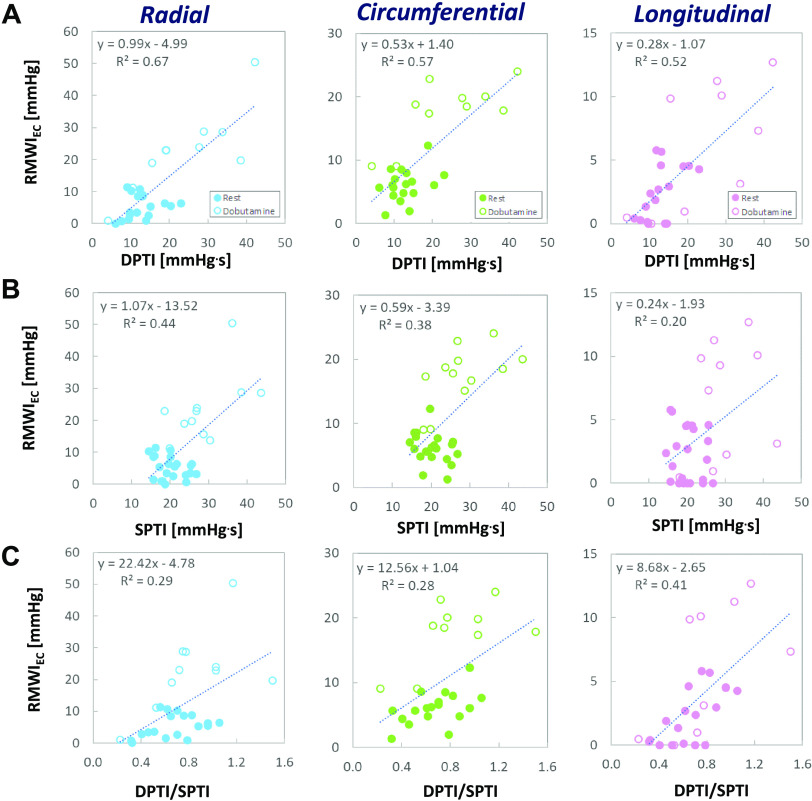
We present a detailed analysis of regional myocardial blood flow and work to better understand the effects of coronary stenoses and low-dose dobutamine stress. Our analysis is based on a unique open-chest model in anesthetized canines that features invasive hemodynamic monitoring, microsphere-based blood flow analysis, and an extensive three-dimensional (3-D) sonomicrometer array that provides multiaxial deformational assessments in the ischemic, border, and remote vascular territories. We use this model to construct regional pressure-strain loops for each territory and quantify the loop subcomponent areas that reflect myocardial work contributing to the ejection of blood and wasted work that does not. We demonstrate that reductions in coronary blood flow markedly alter the shapes and temporal relationships of pressure-strain loops, as well as the magnitudes of their total and subcomponent areas. Specifically, we show that moderate stenoses in the mid-left anterior descending coronary artery decrease regional midventricle myocardial work indices and substantially increase indices of wasted work. In the midventricle, these effects are most pronounced along the radial and longitudinal axes, with more modest effects along the circumferential axis. We further demonstrate that low-dose dobutamine can help to restore or even improve function, but often at the cost of increased wasted work. This detailed, multiaxial analysis provides unique insight into the physiology and mechanics of the heart in the presence of ischemia and low-dose dobutamine, with potential implications in many areas, including the detection and characterization of ischemic heart disease and the use of inotropic support for low cardiac output.NEW & NOTEWORTHY Our unique experimental model assesses cardiac pressure-strain relationships along multiple axes in multiple regions. We demonstrate that moderate coronary stenoses decrease regional myocardial work and increase wasted work and that low-dose dobutamine can help to restore myocardial function, but often with further increases in wasted work. Our findings highlight the significant directional variation of cardiac mechanics and demonstrate potential advantages of pressure-strain analyses over traditional, purely deformational measures, especially in characterizing physiological changes related to dobutamine.
Keywords: coronary stenosis; dobutamine; myocardial strain; myocardial work; pressure-strain.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures

References
-
- Stendahl JC, Parajuli N, Lu A, Boutagy NE, Guerrera N, Alkhalil I, Lin BA, Staib LH, O'Donnell M, Duncan JS, Sinusas AJ. Regional myocardial strain analysis via 2D speckle tracking echocardiography: validation with sonomicrometry and correlation with regional blood flow in the presence of graded coronary stenoses and dobutamine stress. Cardiovasc Ultrasound 18: 2, 2020. doi: 10.1186/s12947-019-0183-x. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources