

International Tuberculum Sellae Meningioma Study: Preoperative Grading Scale to Predict Outcomes and Propensity-Matched Outcomes by Endonasal Versus Transcranial Approach
- PMID: 37418417
- PMCID: PMC12245370
- DOI: 10.1227/neu.0000000000002581
International Tuberculum Sellae Meningioma Study: Preoperative Grading Scale to Predict Outcomes and Propensity-Matched Outcomes by Endonasal Versus Transcranial Approach
Abstract
Background and objectives: Tuberculum sellae meningiomas are resected via an expanded endonasal (EEA) or transcranial approach (TCA). Which approach provides superior outcomes is debated. The Magill-McDermott (M-M) grading scale evaluating tumor size, optic canal invasion, and arterial involvement remains to be validated for outcome prediction. The objective of this study was to validate the M-M scale for predicting visual outcome, extent of resection (EOR), and recurrence, and to use propensity matching by M-M scale to determine whether visual outcome, EOR, or recurrence differ between EEA and TCA.
Methods: Forty-site retrospective study of 947 patients undergoing tuberculum sellae meningiomas resection. Standard statistical methods and propensity matching were used.
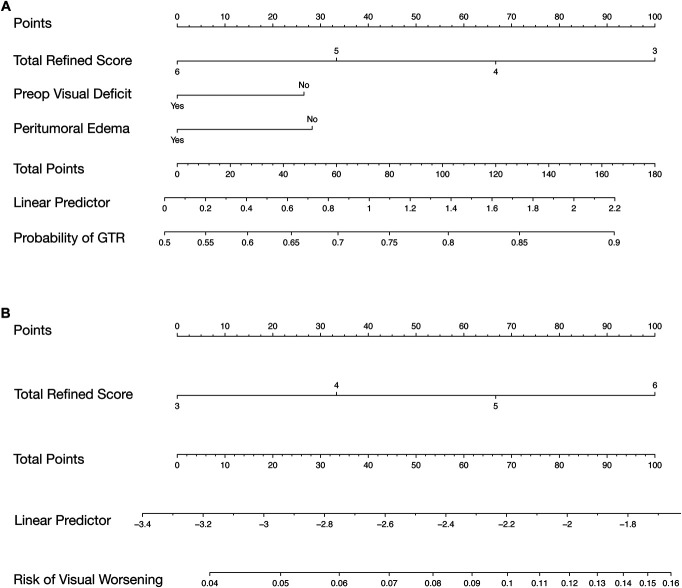
Results: The M-M scale predicted visual worsening (odds ratio [OR]/point: 1.22, 95% CI: 1.02-1.46, P = .0271) and gross total resection (GTR) (OR/point: 0.71, 95% CI: 0.62-0.81, P < .0001), but not recurrence ( P = .4695). The scale was simplified and validated in an independent cohort for predicting visual worsening (OR/point: 2.34, 95% CI: 1.33-4.14, P = .0032) and GTR (OR/point: 0.73, 95% CI: 0.57-0.93, P = .0127), but not recurrence ( P = .2572). In propensity-matched samples, there was no difference in visual worsening ( P = .8757) or recurrence ( P = .5678) between TCA and EEA, but GTR was more likely with TCA (OR: 1.49, 95% CI: 1.02-2.18, P = .0409). Matched patients with preoperative visual deficits who had an EEA were more likely to have visual improvement than those undergoing TCA (72.9% vs 58.4%, P = .0010) with equal rates of visual worsening (EEA 8.0% vs TCA 8.6%, P = .8018).
Conclusion: The refined M-M scale predicts visual worsening and EOR preoperatively. Preoperative visual deficits are more likely to improve after EEA; however, individual tumor features must be considered during nuanced approach selection by experienced neurosurgeons.
Copyright © Congress of Neurological Surgeons 2023. All rights reserved.
Figures




References
-
- Bander ED, Singh H, Ogilvie CB, et al. Endoscopic endonasal versus transcranial approach to tuberculum sellae and planum sphenoidale meningiomas in a similar cohort of patients. J Neurosurg. 2018;128(1):40-48. - PubMed
-
- Magill ST, Morshed RA, Lucas CHG, et al. Tuberculum sellae meningiomas: grading scale to assess surgical outcomes using the transcranial versus transsphenoidal approach. Neurosurg Focus. 2018;44(4):e9. - PubMed
-
- Setty P, Fernandez-Miranda JC, Wang EW, Snyderman CH, Gardner PA. Residual and recurrent disease following endoscopic endonasal approach as a reflection of anatomic limitation for the resection of midline anterior skull base meningiomas. Oper Neurosurg. 2021;21(4):207-216. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
