

Sleep Apnea Physiological Burdens and Cardiovascular Morbidity and Mortality
- PMID: 37418748
- PMCID: PMC10563185
- DOI: 10.1164/rccm.202209-1808OC
Sleep Apnea Physiological Burdens and Cardiovascular Morbidity and Mortality
Abstract
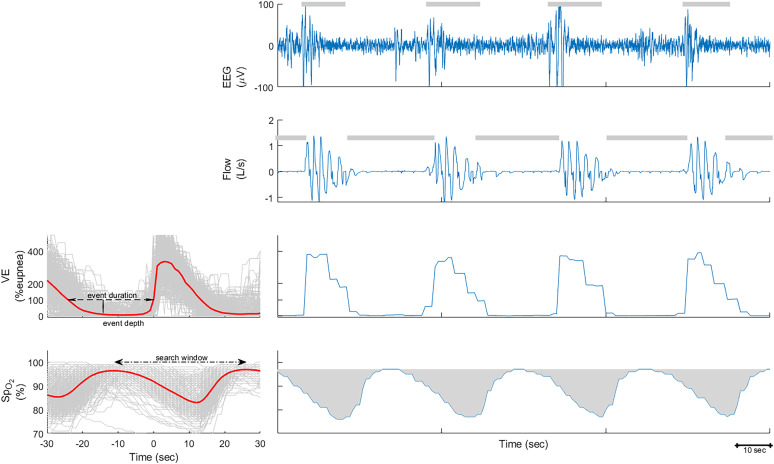
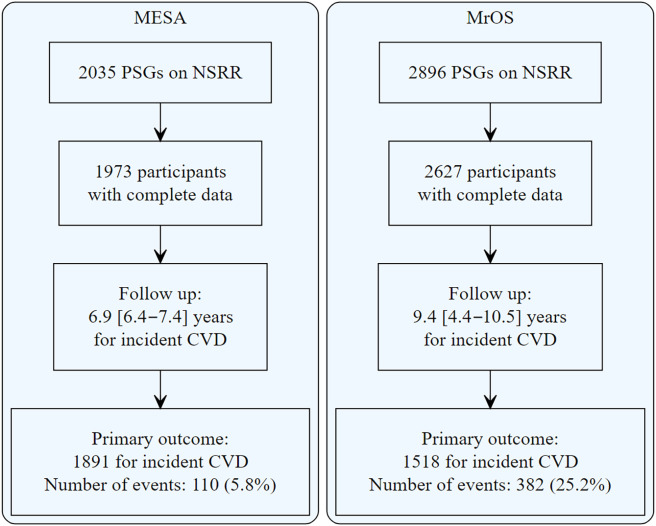
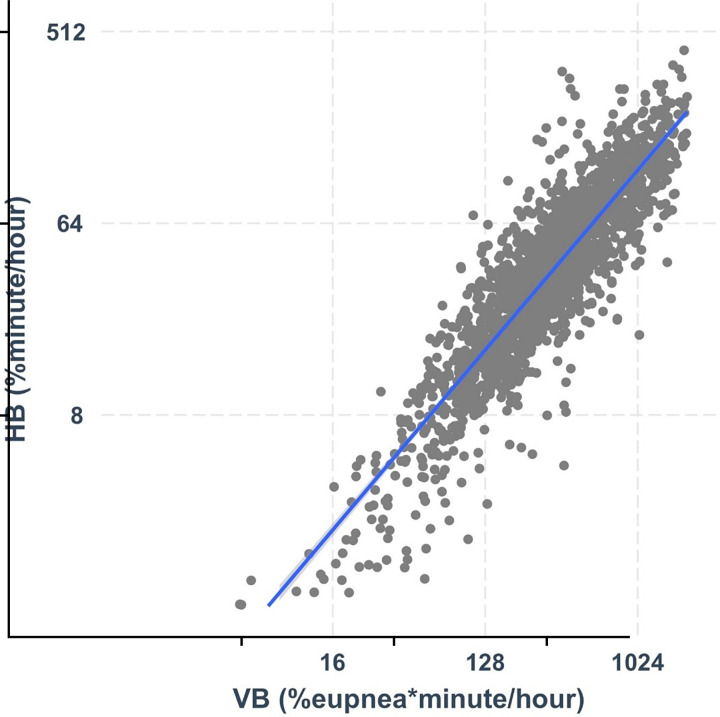
Rationale: Obstructive sleep apnea is characterized by frequent reductions in ventilation, leading to oxygen desaturations and/or arousals. Objectives: In this study, association of hypoxic burden with incident cardiovascular disease (CVD) was examined and compared with that of "ventilatory burden" and "arousal burden." Finally, we assessed the extent to which the ventilatory burden, visceral obesity, and lung function explain variations in hypoxic burden. Methods: Hypoxic, ventilatory, and arousal burdens were measured from baseline polysomnograms in the Multi-Ethnic Study of Atherosclerosis (MESA) and the Osteoporotic Fractures in Men (MrOS) studies. Ventilatory burden was defined as event-specific area under ventilation signal (mean normalized, area under the mean), and arousal burden was defined as the normalized cumulative duration of all arousals. The adjusted hazard ratios for incident CVD and mortality were calculated. Exploratory analyses quantified contributions to hypoxic burden of ventilatory burden, baseline oxygen saturation as measured by pulse oximetry, visceral obesity, and spirometry parameters. Measurements and Main Results: Hypoxic and ventilatory burdens were significantly associated with incident CVD (adjusted hazard ratio [95% confidence interval] per 1 SD increase in hypoxic burden: MESA, 1.45 [1.14, 1.84]; MrOS, 1.13 [1.02, 1.26]; ventilatory burden: MESA, 1.38 [1.11, 1.72]; MrOS, 1.12 [1.01, 1.25]), whereas arousal burden was not. Similar associations with mortality were also observed. Finally, 78% of variation in hypoxic burden was explained by ventilatory burden, whereas other factors explained only <2% of variation. Conclusions: Hypoxic and ventilatory burden predicted CVD morbidity and mortality in two population-based studies. Hypoxic burden is minimally affected by measures of adiposity and captures the risk attributable to ventilatory burden of obstructive sleep apnea rather than a tendency to desaturate.
Keywords: arousals; cardiovascular disease; hypoxic burden; obstructive sleep apnea; ventilatory burden.
Figures
Comment in
-
The Influence of Physiologic Burdens Related to Obstructive Sleep Apnea on Cardiovascular Outcomes.Am J Respir Crit Care Med. 2023 Oct 1;208(7):752-754. doi: 10.1164/rccm.202307-1243ED. Am J Respir Crit Care Med. 2023. PMID: 37610456 Free PMC article. No abstract available.
References
-
- Veasey SC, Rosen IM. Obstructive sleep apnea in adults. N Engl J Med . 2019;380:1442–1449. - PubMed
-
- Kulkas A, Duce B, Leppänen T, Hukins C, Töyräs J. Severity of desaturation events differs between hypopnea and obstructive apnea events and is modulated by their duration in obstructive sleep apnea. Sleep Breath . 2017;21:829–835. - PubMed
-
- Leppänen T, Kulkas A, Mervaala E, Töyräs J. Increase in body mass index decreases duration of apneas and hypopneas in obstructive sleep apnea. Respir Care . 2019;64:77–84. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- R01 HL071194/HL/NHLBI NIH HHS/United States
- UL1 TR002369/TR/NCATS NIH HHS/United States
- R01 AG070867/AG/NIA NIH HHS/United States
- U01 AG042145/AG/NIA NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL158765/HL/NHLBI NIH HHS/United States
- U01 AG042168/AG/NIA NIH HHS/United States
- R01 HL070841/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- R24 HL114473/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- U01 AG042139/AG/NIA NIH HHS/United States
- P50 HL056984/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- R01 HL070848/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- R01 HL070847/HL/NHLBI NIH HHS/United States
- R01 HL070842/HL/NHLBI NIH HHS/United States
- R01 AG066671/AG/NIA NIH HHS/United States
- U01 AG042124/AG/NIA NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- R01 HL070838/HL/NHLBI NIH HHS/United States
- R21 HL161766/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- R01 HL070839/HL/NHLBI NIH HHS/United States
- R01 HL153874/HL/NHLBI NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- R01 HL070837/HL/NHLBI NIH HHS/United States
- U01 AG042143/AG/NIA NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
