

Predictors of outcome for treatment of enterovaginal fistula : Therapeutical strategies for treatment
- PMID: 37420132
- PMCID: PMC10329052
- DOI: 10.1007/s00384-023-04453-2
Predictors of outcome for treatment of enterovaginal fistula : Therapeutical strategies for treatment
Abstract
Background: Enterovaginal fistulas represent a serious complication of various diseases and therapeutic procedures, often associated with complicated clinical courses and massive impairment of quality of life. As underlying conditions and procedures are multifarious, therapeutic approaches are challenging and have to be tailored individually. As the therapeutic management is complex and individualized, multiple surgical interventions might be necessary.
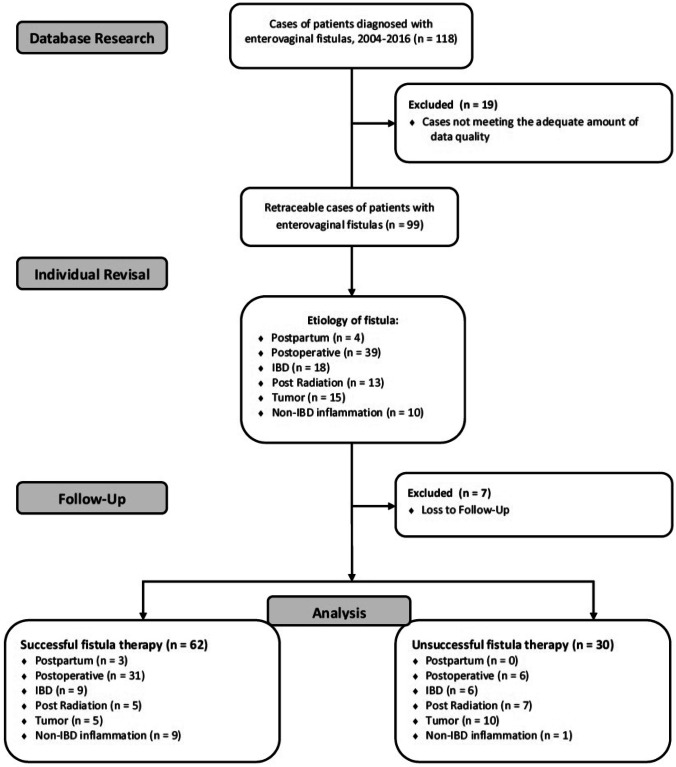
Methods: The aim of this study was to identify possible predictors for outcome in the treatment enterovaginal fistula patients. The study was realized as a retrospective analysis. Ninety-two patients treated with enterovaginal fistulas between 2004 and 2016 were analyzed. Patient characteristics, therapeutic data, and endoscopic findings were stratified according to etiology, closure rate and time, as well as recurrence of fistula. Main outcome measure was the overall rate of fistula closure.
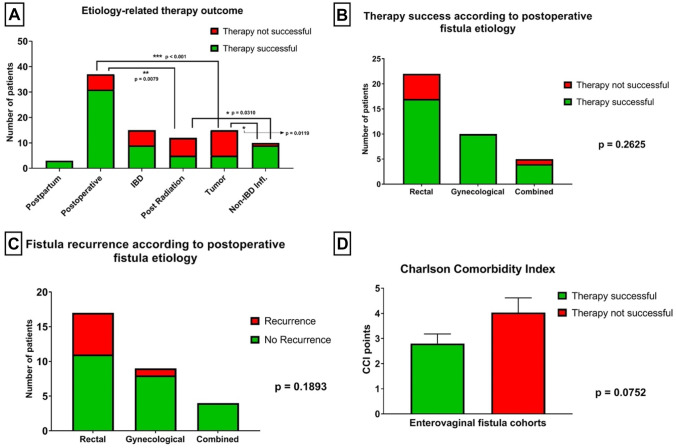
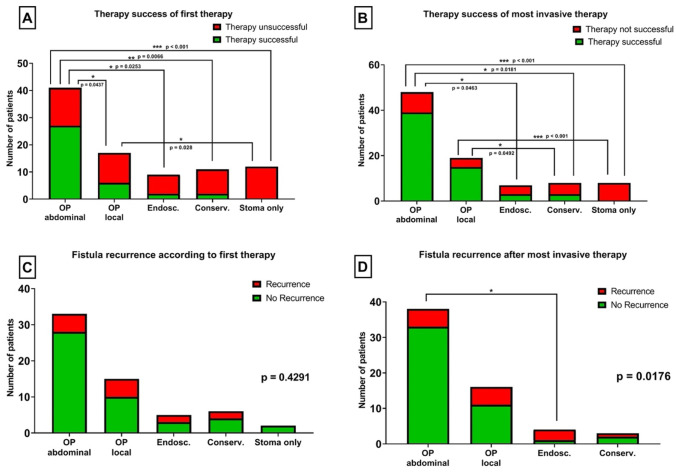
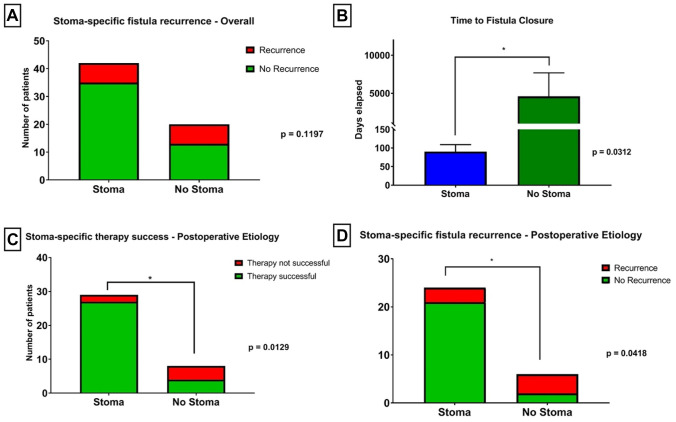
Results: Overall therapeutic success rate was 67.4%. Postoperatively derived fistulas were most frequent (40.2%), mainly after rectal surgery (59.5%). Postoperative and non-IBD-inflammation associated fistulas had better outcome than IBD-, radiotherapy-, and tumor-related fistulas (p = 0.001). Successful fistula closure was observed more frequently after radical surgical interventions, best results observed after transabdominal surgery (p < 0.001). Fistula recurrence was also less frequently observed after radical surgical therapies (p = 0.029). A temporary stoma was associated with higher incidence of fistula closure (p = 0.013) and lower incidence of fistula recurrence (p = 0.042) in the postoperative subgroup, as well as shortened therapy period in all groups (p = 0.031).
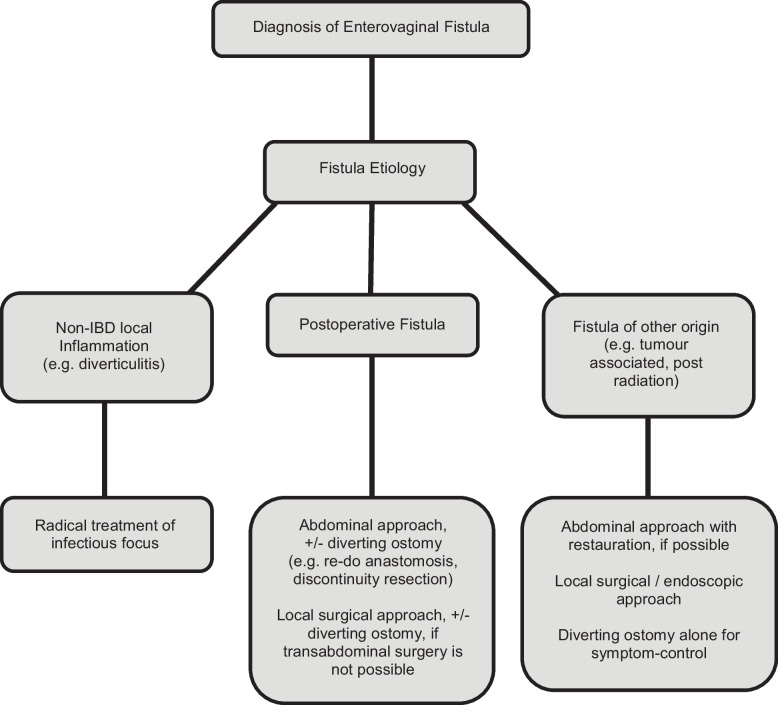
Conclusion: Enterovaginal fistulas are a result of various etiologies, and treatment should be adjusted accordingly. A very sustainable, rapid, and persistent therapeutic success can be expected after radical surgical approaches with temporary diverting stoma. This is especially true for postoperatively derived fistulas.
Keywords: Enterovaginal fistulas; Rectovaginal fistulas; Therapeutic outcome for enterovaginal fistulas.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Gracilis muscle transposition in complex anorectal fistulas of diverse types and etiologies: long-term results of 60 cases.Int J Colorectal Dis. 2023 Jan 18;38(1):16. doi: 10.1007/s00384-022-04293-6. Int J Colorectal Dis. 2023. PMID: 36652018 Free PMC article.
-
Gracilis Flap Repair for Reoperative Rectovaginal Fistula.Dis Colon Rectum. 2023 Jan 1;66(1):113-117. doi: 10.1097/DCR.0000000000002249. Epub 2022 Oct 25. Dis Colon Rectum. 2023. PMID: 34759248
-
Treatment of recurrent rectovaginal/pouch-vaginal fistulas by gracilis muscle transposition - a single center experience.J Visc Surg. 2013 Dec;150(6):379-82. doi: 10.1016/j.jviscsurg.2013.08.002. Epub 2013 Oct 18. J Visc Surg. 2013. PMID: 24144724
-
Rectovaginal fistula in Crohn's disease.Dis Colon Rectum. 2007 Dec;50(12):2215-22. doi: 10.1007/s10350-007-9057-7. Epub 2007 Sep 11. Dis Colon Rectum. 2007. PMID: 17846837 Review.
-
Management of rectovaginal fistulas and patient outcome.Expert Rev Gastroenterol Hepatol. 2017 May;11(5):461-471. doi: 10.1080/17474124.2017.1296355. Epub 2017 Mar 1. Expert Rev Gastroenterol Hepatol. 2017. PMID: 28276809 Review.
Cited by
-
[Rectovaginal fistulas : Differentiated diagnostics and treatment].Chirurgie (Heidelb). 2024 Dec;95(12):1027-1040. doi: 10.1007/s00104-024-02151-5. Epub 2024 Sep 16. Chirurgie (Heidelb). 2024. PMID: 39283323 Review. German.
-
Endoscopic Deployment of Cardiac Septal Occluder Device to Close an Enterovaginal Fistula.ACG Case Rep J. 2024 Jul 27;11(8):e01452. doi: 10.14309/crj.0000000000001452. eCollection 2024 Aug. ACG Case Rep J. 2024. PMID: 39081303 Free PMC article.
-
Successful Fistula Closure After Treatment with Colostomy and Infliximab in a Patient with Ulcerative Colitis Complicated by Rectovaginal Fistula.Biologics. 2024 May 6;18:107-113. doi: 10.2147/BTT.S457300. eCollection 2024. Biologics. 2024. PMID: 38736705 Free PMC article.
-
Postoperative rectovaginal fistula: stoma may not be necessary-a French retrospective cohort.Tech Coloproctol. 2024 Oct 3;28(1):138. doi: 10.1007/s10151-024-03013-2. Tech Coloproctol. 2024. PMID: 39361109 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
