

Long term outcomes and causal modelling of compulsory inpatient and outpatient mental health care using Norwegian registry data: Protocol for a controversies in psychiatry research project
- PMID: 37421245
- PMCID: PMC10807697
- DOI: 10.1002/mpr.1980
Long term outcomes and causal modelling of compulsory inpatient and outpatient mental health care using Norwegian registry data: Protocol for a controversies in psychiatry research project
Abstract
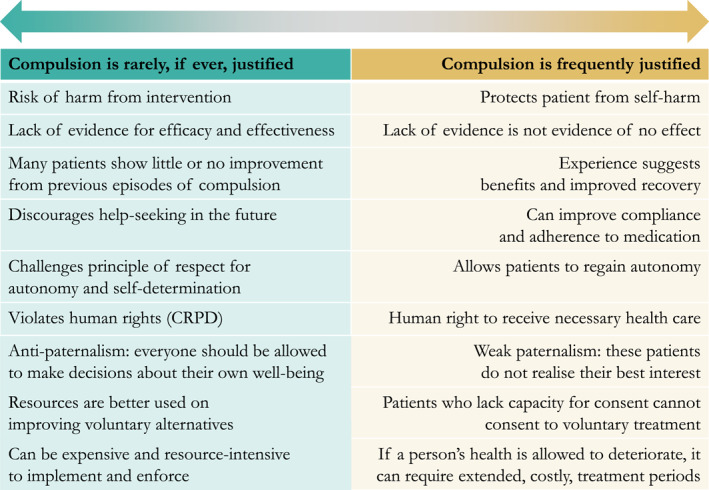
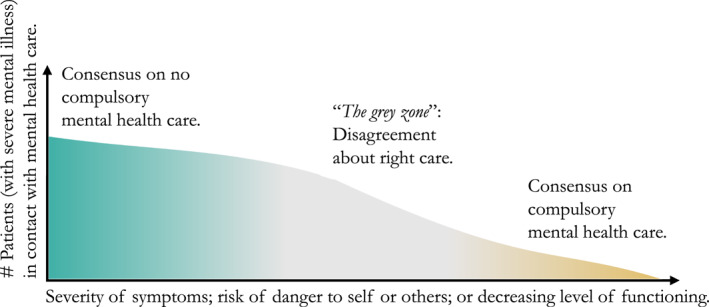
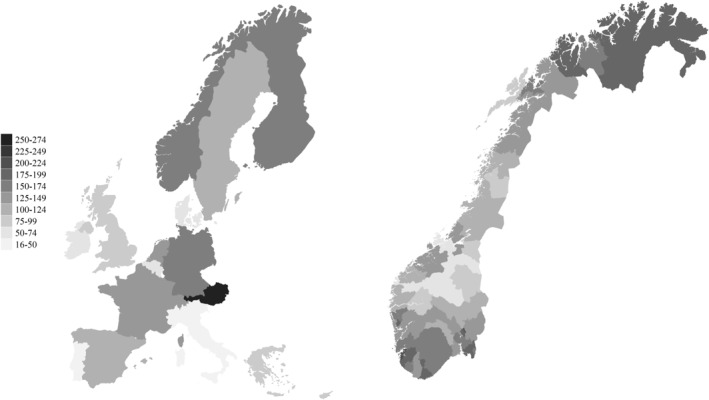
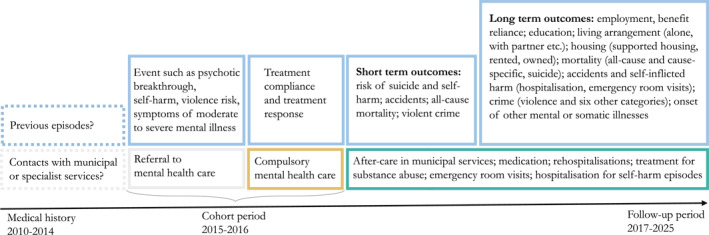
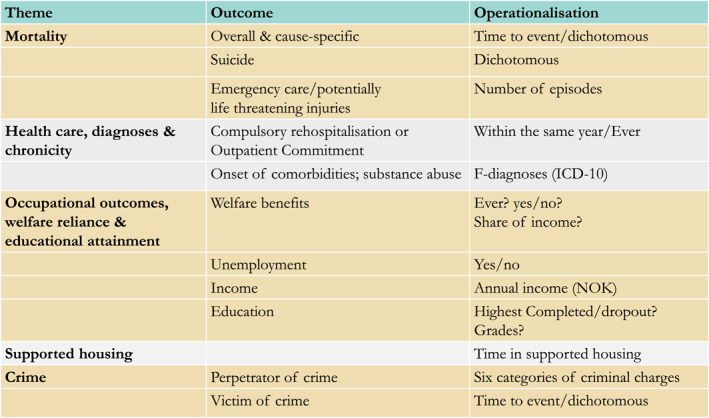
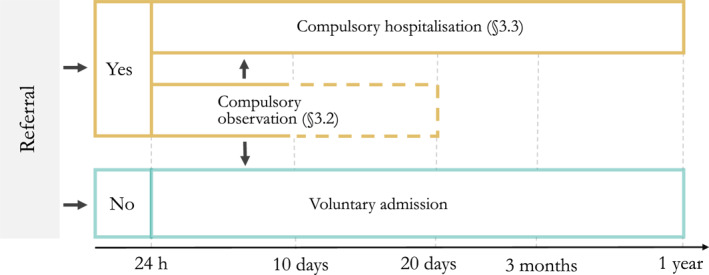
Objectives: Compulsory mental health care includes compulsory hospitalisation and outpatient commitment with medication treatment without consent. Uncertain evidence of the effects of compulsory care contributes to large geographical variations and a controversy on its use. Some argue that compulsion can rarely be justified and should be reduced to an absolute minimum, while others claim compulsion can more frequently be justified. The limited evidence base has contributed to variations in care that raise issues about the quality/appropriateness of care as well as ethical concerns. To address the question whether compulsory mental health care results in superior, worse or equivalent outcomes for patients, this project will utilise registry-based longitudinal data to examine the effect of compulsory inpatient and outpatient care on multiple outcomes, including suicide and overall mortality; emergency care/injuries; crime and victimisation; and participation in the labour force and welfare dependency.
Methods: By using the natural variation in health providers' preference for compulsory care as a source of quasi-randomisation we will estimate causal effects of compulsory care on short- and long-term trajectories.
Conclusions: This project will provide valuable insights for service providers and policy makers in facilitating high quality clinical care pathways for a high risk population group.
Keywords: causal inference; coercion; compulsion; compulsory mental health care; geographical variation; instrumental variables; psychiatric epidemiology.
© 2023 The Authors. International Journal of Methods in Psychiatric Research published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Aasland, O. G. , Husum, T. L. , Førde, R. , & Pedersen, R. (2018). Between authoritarian and dialogical approaches: Attitudes and opinions on coercion among professionals in mental health and addiction care in Norway. International Journal of Law and Psychiatry, 57, 106–112. 10.1016/j.ijlp.2018.02.005 - DOI - PubMed
-
- Angrist, J. D. , Imbens, G. W. , & Rubin, D. B. (1996). Identification of causal effects using instrumental variables. Journal of the American Statistical Association, 91(434), 444–455. 10.1080/01621459.1996.10476902 - DOI
-
- Bagby, R. M. , Thompson, J. S. , Dickens, S. E. , & Nohara, M. (1991). Decision making in psychiatric civil commitment: An experimental analysis. American Journal of Psychiatry, 148(1), 28–33. - PubMed
-
- Bale M., Holsen M., Osvoll K. I., Bedane H. K., Skrede O. Healthcare Atlas for Mental Healthcare and Substance Abuse Treatment. Overview and analysis of use of mental healthcare and interdisciplinary specialised addiction services in Norway for the years 2014‐2018 [Internet]. Helse Førde HF; 2021. Retrieved from: https://helseatlas.no/sites/default/files/mhc_report.pdf
-
- Barkhuizen, W. , Cullen, A. E. , Shetty, H. , Pritchard, M. , Stewart, R. , McGuire, P. , & Patel, R. (2020). Community treatment orders and associations with readmission rates and duration of psychiatric hospital admission: A controlled electronic case register study. BMJ Open, 10(3), e035121. 10.1136/bmjopen-2019-035121 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
