

Individual Trajectories of Health Status During the First Year of Discharge From Hospitalization for Heart Failure and Their Associations With Death in the Following Years
- PMID: 37421271
- PMCID: PMC10382098
- DOI: 10.1161/JAHA.122.028782
Individual Trajectories of Health Status During the First Year of Discharge From Hospitalization for Heart Failure and Their Associations With Death in the Following Years
Abstract
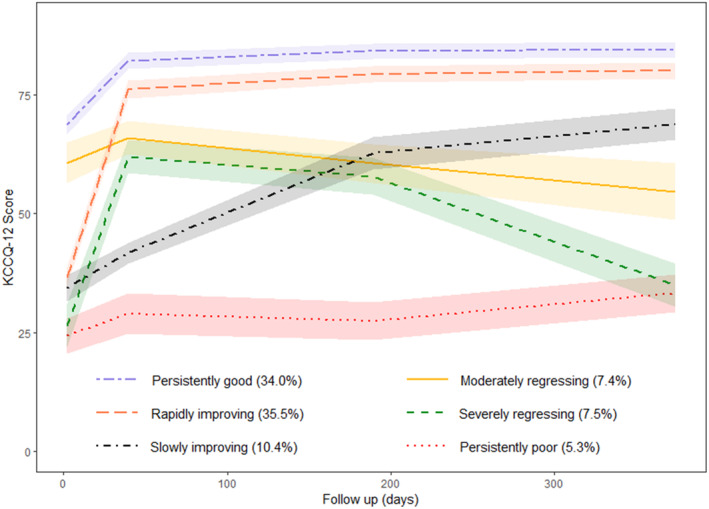
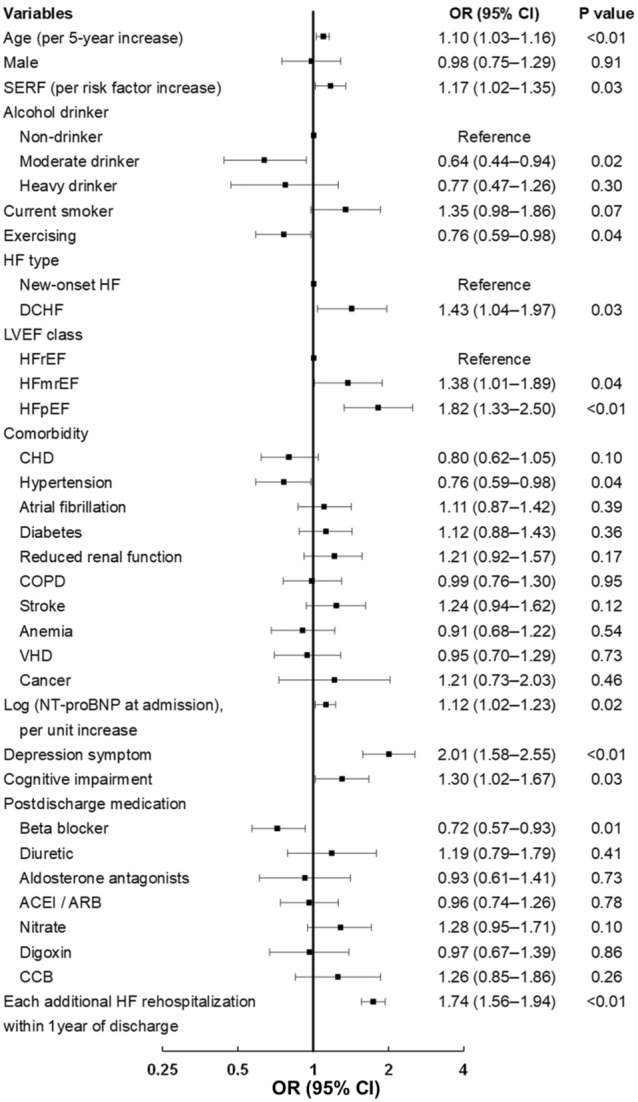
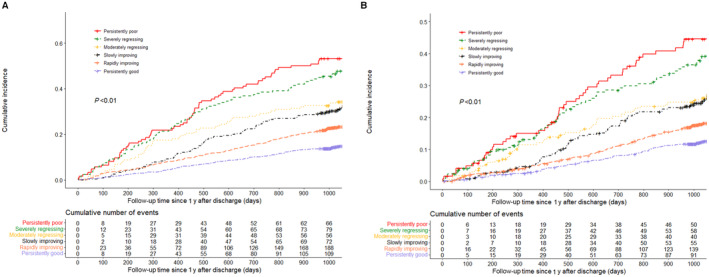
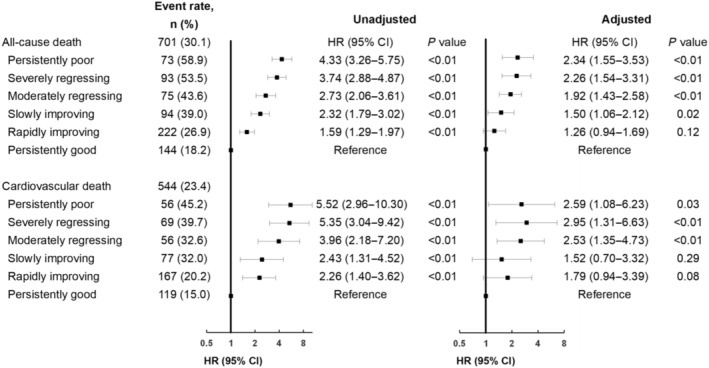
Background Improving health status is one of the major goals in the management of heart failure (HF). However, little is known about the long-term individual trajectories of health status in patients with acute HF after discharge. Methods and Results We enrolled 2328 patients hospitalized for HF from 51 hospitals prospectively and measured their health status via the Kansas City Cardiomyopathy Questionnaire-12 at admission and 1, 6, and 12 months after discharge, respectively. The median age of the patients included was 66 years, and 63.3% were men. Six patterns of Kansas City Cardiomyopathy Questionnaire-12 trajectories were identified by a latent class trajectory model: persistently good (34.0%), rapidly improving (35.5%), slowly improving (10.4%), moderately regressing (7.4%), severely regressing (7.5%), and persistently poor (5.3%). Advanced age, decompensated chronic HF, HF with mildly reduced ejection fraction, HF with preserved ejection fraction, depression symptoms, cognitive impairment, and each additional HF rehospitalization within 1 year of discharge were associated with unfavorable health status (moderately regressing, severely regressing, and persistently poor) (P<0.05). Compared with the pattern of persistently good, slowly improving (hazard ratio [HR], 1.50 [95% CI, 1.06-2.12]), moderately regressing (HR, 1.92 [1.43-2.58]), severely regressing (HR, 2.26 [1.54-3.31]), and persistently poor (HR, 2.34 [1.55-3.53]) were associated with increased risks of all-cause death. Conclusions One-fifth of 1-year survivors after hospitalization for HF experienced unfavorable health status trajectories and had a substantially increased risk of death during the following years. Our findings help inform the understanding of disease progression from a patient perception perspective and its relationship with long-term survival. Registration URL: https://www.clinicaltrials.gov; unique identifier: NCT02878811.
Keywords: acute heart failure; death; health status; prognosis.
Figures
References
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, Abbastabar H, Abd‐Allah F, Abdela J, Abdelalim A, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Johansson I, Joseph P, Balasubramanian K, McMurray JJV, Lund LH, Ezekowitz JA, Kamath D, Alhabib K, Bayes‐Genis A, Budaj A, et al. Health‐related quality of life and mortality in heart failure: the global congestive heart failure study of 23 000 patients from 40 countries. Circulation. 2021;143:2129–2142. doi: 10.1161/CIRCULATIONAHA.120.050850 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
