

Sex Differences in the Effectiveness of Angiotensin-Converting Enzyme Inhibitors, Angiotensin II Receptor Blockers, and Sacubitril-Valsartan for the Treatment of Heart Failure
- PMID: 37421275
- PMCID: PMC10382087
- DOI: 10.1161/JAHA.122.028865
Sex Differences in the Effectiveness of Angiotensin-Converting Enzyme Inhibitors, Angiotensin II Receptor Blockers, and Sacubitril-Valsartan for the Treatment of Heart Failure
Abstract
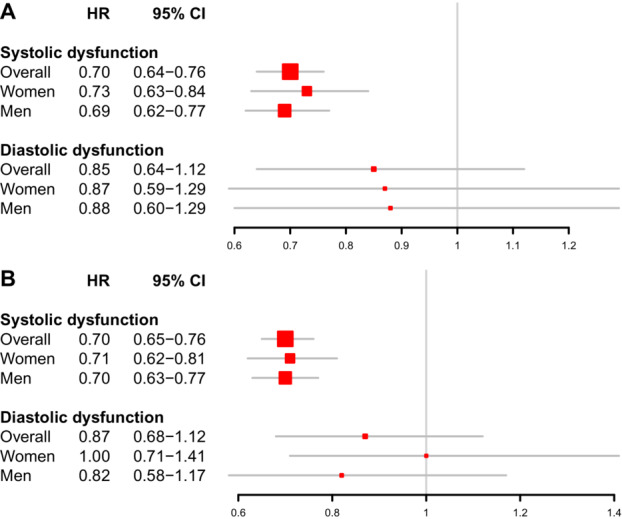
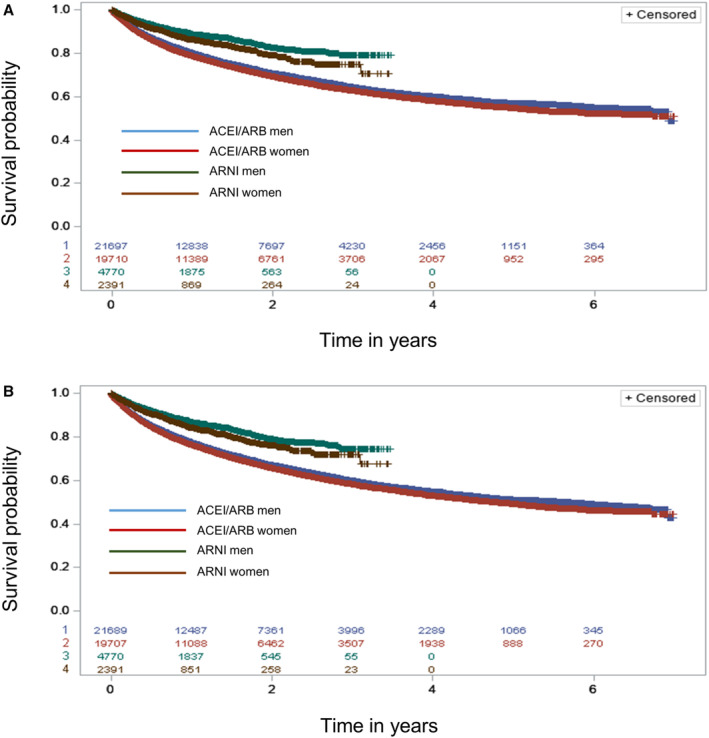
Background PARAGON-HF (Efficacy and Safety of LCZ696 Compared to Valsartan, on Morbidity and Mortality in Heart Failure Patients With Preserved Ejection Fraction) suggested a potential benefit of sacubitril-valsartan in women with preserved ejection fraction. Among patients with heart failure previously treated with angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs), we studied whether effectiveness of treatment with sacubitril-valsartan compared with ACEI/ARB monotherapy differed between men and women for both preserved and reduced ejection fraction. Methods and Results Data were derived from the Truven Health MarketScan Databases between January 1, 2011, and December 31, 2018. We included patients with a primary diagnosis of heart failure on treatment with ACEIs, ARBs, or sacubitril-valsartan on the basis of the first prescription after diagnosis. A total of 7181 patients treated with sacubitril-valsartan, 25 408 patients using an ACEI, and 16 177 patients treated with ARBs were included. A total of 790 readmissions or deaths occurred among 7181 patients in the sacubitril-valsartan group and 11 901 events in 41 585 patients treated with an ACEI/ARB. Adjusted for covariates, the hazard ratio (HR) for treatment with sacubitril-valsartan compared with an ACEI or ARB was 0.74 (95% CI, 0.68-0.80). The protective effect of sacubitril-valsartan was evident for men and women (women: HR, 0.75 [95% CI, 0.66-0.86]; P<0.01; men: HR, 0.71 [95% CI, 0.64-0.79]; P<0.01; P interaction 0.03). A protective effect for both sexes was seen only among those with systolic dysfunction. Conclusions Treatment with sacubitril-valsartan is more effective at reducing death and admission to the hospital for heart failure compared with ACEIs/ARBs similarly among men and women with systolic dysfunction; sex differences in the effectiveness of sacubitril-valsartan in diastolic dysfunction requires further investigation.
Keywords: heart failure; observational study; sacubitril–valsartan; sex differences.
Figures
Similar articles
-
Efficacy and Safety of Sacubitril/Valsartan Therapy for Acute Decompensated Heart Failure with Reduced Ejection Fraction during the Vulnerable Phase: A Multicenter, Assessor-Blinded, Prospective, Observational, Cohort Study.Cardiology. 2021;146(3):335-344. doi: 10.1159/000512418. Epub 2021 Mar 29. Cardiology. 2021. PMID: 33780933
-
Sacubitril/valsartan improves all-cause mortality in heart failure patients with reduced ejection fraction and chronic kidney disease.Cardiovasc Drugs Ther. 2024 Jun;38(3):505-515. doi: 10.1007/s10557-022-07421-0. Epub 2023 Jan 7. Cardiovasc Drugs Ther. 2024. PMID: 36609948 Free PMC article.
-
Comparative Effectiveness of Sacubitril-Valsartan Versus ACE/ARB Therapy in Heart Failure With Reduced Ejection Fraction.JACC Heart Fail. 2020 Jan;8(1):43-54. doi: 10.1016/j.jchf.2019.08.003. Epub 2019 Dec 11. JACC Heart Fail. 2020. PMID: 31838035 Free PMC article.
-
Effectiveness and Safety of Sacubitril/Valsartan in Heart Failure with Preserved Ejection Fraction: A Systematic Review and Meta-Analysis.Altern Ther Health Med. 2024 Apr;30(4):190-197. Altern Ther Health Med. 2024. PMID: 37917889
-
Effect of sacubitril/valsartan and ACEI/ARB on glycaemia and the development of diabetes: a systematic review and meta-analysis of randomised controlled trials.BMC Med. 2022 Dec 17;20(1):487. doi: 10.1186/s12916-022-02682-w. BMC Med. 2022. PMID: 36527023 Free PMC article.
Cited by
-
MAGGIC risk score and drug-related adverse events of sacubitril/valsartan: Insights from the REVIEW-HF registry.Int J Cardiol Heart Vasc. 2025 May 10;59:101702. doi: 10.1016/j.ijcha.2025.101702. eCollection 2025 Aug. Int J Cardiol Heart Vasc. 2025. PMID: 40476175 Free PMC article.
-
Sex Disparities in Cardiovascular Disease.Methodist Debakey Cardiovasc J. 2024 Mar 14;20(2):107-119. doi: 10.14797/mdcvj.1328. eCollection 2024. Methodist Debakey Cardiovasc J. 2024. PMID: 38495656 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
