

Frailty, Treatments, and Outcomes in Older Patients With Myocardial Infarction: A Nationwide Registry-Based Study
- PMID: 37421279
- PMCID: PMC10382124
- DOI: 10.1161/JAHA.123.030561
Frailty, Treatments, and Outcomes in Older Patients With Myocardial Infarction: A Nationwide Registry-Based Study
Abstract
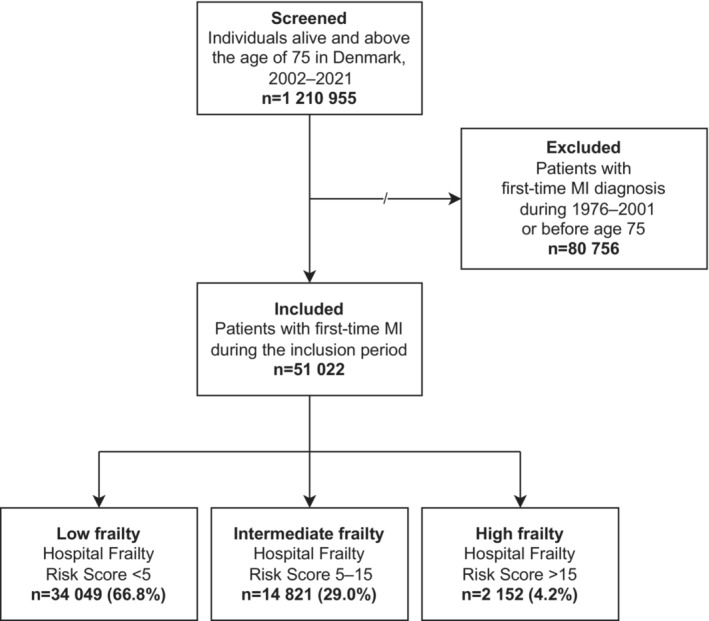
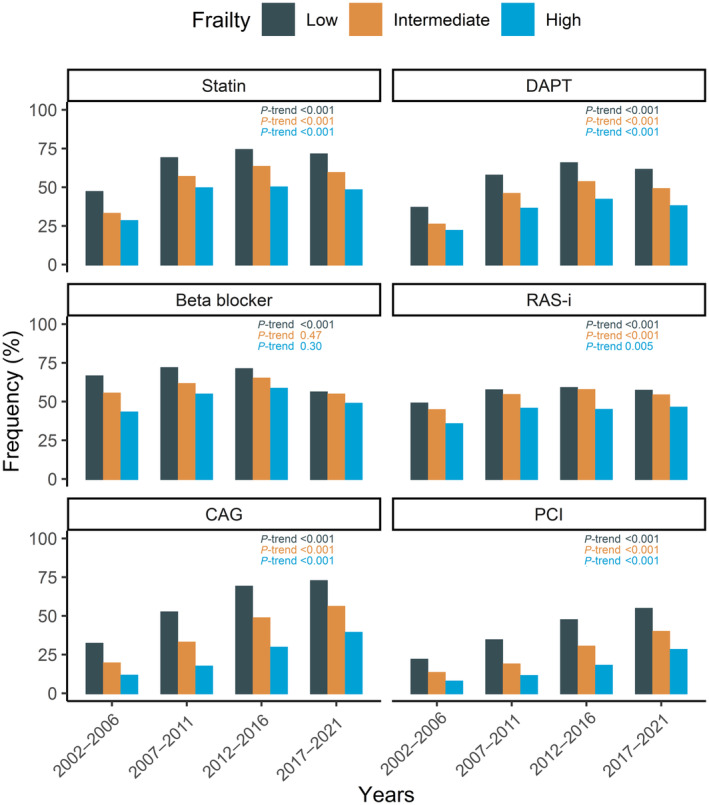
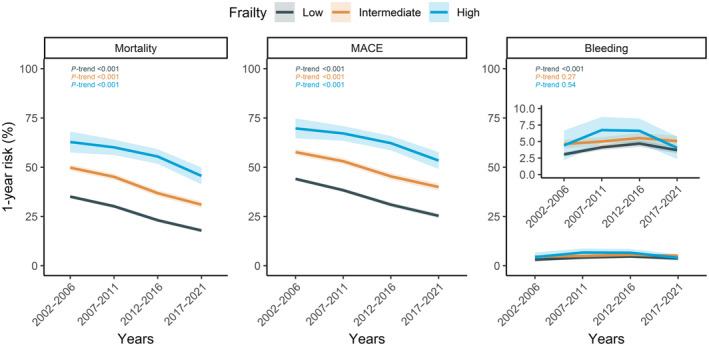
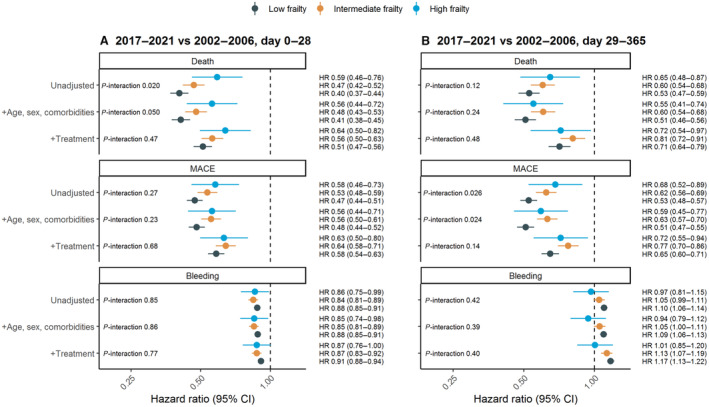
Background Guidelines recommend that patients with myocardial infarction (MI) receive equal care regardless of age. However, withholding treatment may be justified in elderly and frail patients. This study aimed to investigate trends in treatments and outcomes of older patients with MI according to frailty. Methods and Results All patients aged ≥75 years with first-time MI during 2002 to 2021 were identified through Danish nationwide registries. Frailty was categorized using the Hospital Frailty Risk Score. One-year risk and hazard ratios (HRs) for days 0 to 28 and 29 to 365 were calculated for all-cause death. A total of 51 022 patients with MI were included (median, 82 years; 50.2% women). Intermediate/high frailty increased from 26.7% in 2002 to 2006 to 37.1% in 2017 to 2021. Use of treatment increased substantially regardless of frailty: for example, 28.1% to 48.0% (statins), 21.8% to 33.7% (dual antiplatelet therapy), and 7.6% to 28.0% (percutaneous coronary intervention) for high frailty (all P-trend <0.001). One-year death decreased for low frailty (35.1%-17.9%), intermediate frailty (49.8%-31.0%), and high frailty (62.8%-45.6%), all P-trend <0.001. Age- and sex-adjusted 29- to 365-day HRs (2017-2021 versus 2002-2006) were 0.53 (0.48-0.59), 0.62 (0.55-0.70), and 0.62 (0.46-0.83) for low, intermediate, and high frailty, respectively (P-interaction=0.23). When additionally adjusted for treatment, HRs attenuated to 0.74 (0.67-0.83), 0.83 (0.74-0.94), and 0.78 (0.58-1.05), respectively, indicating that increased use of treatment may account partially for the observed improvements. Conclusions Use of guideline-based treatments and outcomes improved concomitantly in older patients with MI, irrespective of frailty. These results indicate that guideline-based management of MI may be reasonable in the elderly and frail.
Keywords: frailty; guidelines; myocardial infarction; old; outcomes; trends.
Figures
Similar articles
-
Frailty Among Older Adults With Acute Myocardial Infarction and Outcomes From Percutaneous Coronary Interventions.J Am Heart Assoc. 2019 Sep 3;8(17):e013686. doi: 10.1161/JAHA.119.013686. Epub 2019 Aug 31. J Am Heart Assoc. 2019. PMID: 31475601 Free PMC article.
-
The Association of Frailty With In-Hospital Bleeding Among Older Adults With Acute Myocardial Infarction: Insights From the ACTION Registry.JACC Cardiovasc Interv. 2018 Nov 26;11(22):2287-2296. doi: 10.1016/j.jcin.2018.08.028. JACC Cardiovasc Interv. 2018. PMID: 30466828 Free PMC article.
-
Frailty and Outcomes After Myocardial Infarction: Insights From the CONCORDANCE Registry.J Am Heart Assoc. 2018 Sep 18;7(18):e009859. doi: 10.1161/JAHA.118.009859. J Am Heart Assoc. 2018. PMID: 30371219 Free PMC article.
-
Clinical outcomes of nonagenarians with acute myocardial infarction who undergo percutaneous coronary intervention.Eur Heart J Acute Cardiovasc Care. 2020 Aug;9(5):488-495. doi: 10.1177/2048872620921596. Epub 2020 Apr 23. Eur Heart J Acute Cardiovasc Care. 2020. PMID: 32324045
-
Acute coronary care in the elderly, part I: Non-ST-segment-elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology.Circulation. 2007 May 15;115(19):2549-69. doi: 10.1161/CIRCULATIONAHA.107.182615. Circulation. 2007. PMID: 17502590 Review.
Cited by
-
Frailty prevalence, invasive treatment frequency, and in-hospital outcome in patients hospitalized for acute coronary syndrome in Germany (2005-2022): a nationwide registry study.Lancet Reg Health Eur. 2024 Dec 9;49:101168. doi: 10.1016/j.lanepe.2024.101168. eCollection 2025 Feb. Lancet Reg Health Eur. 2024. PMID: 39737370 Free PMC article.
-
Linking Myocardial Infarction and Frailty Status at Old Age in Europe: Moderation Effects of Country and Gender.J Cardiovasc Dev Dis. 2024 Jun 8;11(6):176. doi: 10.3390/jcdd11060176. J Cardiovasc Dev Dis. 2024. PMID: 38921676 Free PMC article.
-
Epigenetic Biomarkers of Cardiovascular Risk in Frail Patients-A Scope Review.Curr Issues Mol Biol. 2025 Jun 5;47(6):422. doi: 10.3390/cimb47060422. Curr Issues Mol Biol. 2025. PMID: 40699821 Free PMC article. Review.
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli‐Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Collet J‐P, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST‐segment elevation: the Task Force for the management of acute coronary syndromes in patients presenting without persistent ST‐segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2021;42:1289–1367. doi: 10.1093/eurheartj/ehaa575 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
