

Myocardial Infarction Across COVID-19 Pandemic Phases: Insights From the Veterans Health Affairs System
- PMID: 37421288
- PMCID: PMC10382121
- DOI: 10.1161/JAHA.123.029910
Myocardial Infarction Across COVID-19 Pandemic Phases: Insights From the Veterans Health Affairs System
Abstract
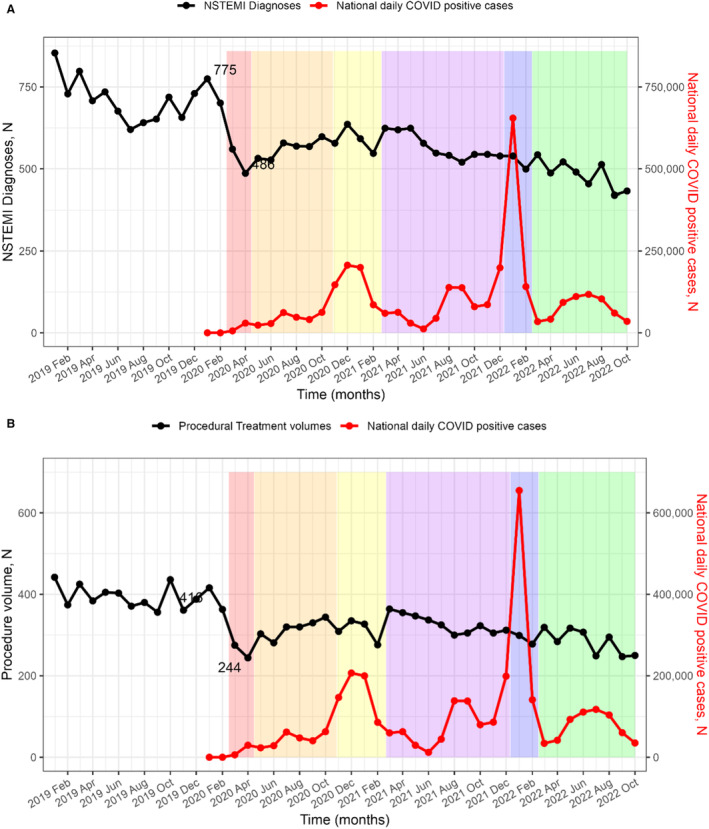
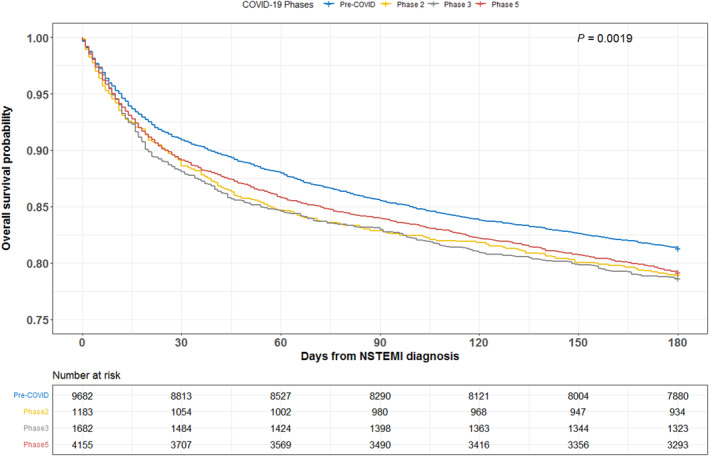
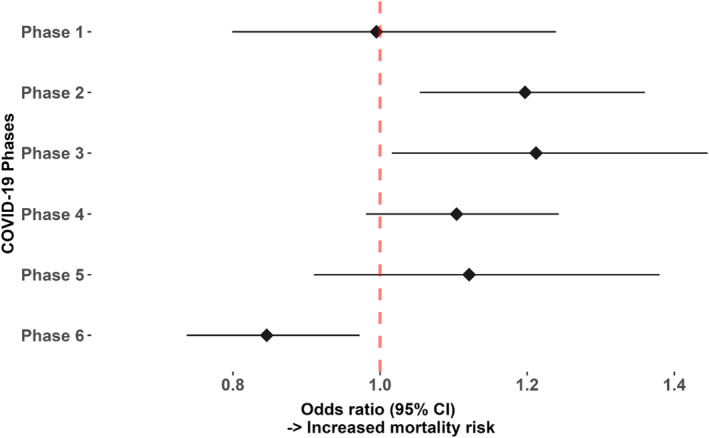
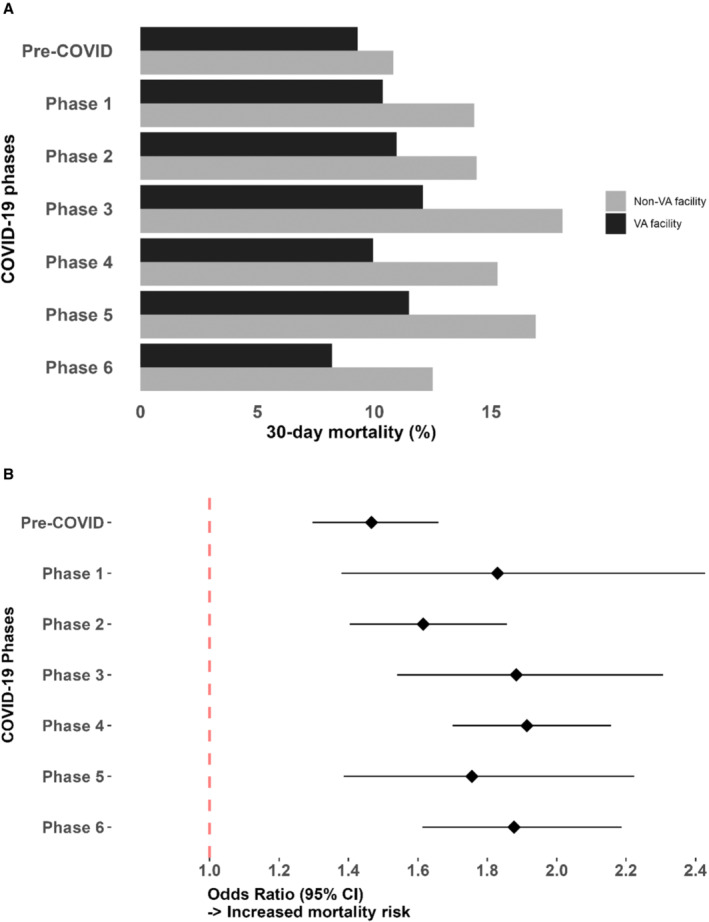
Background Cardiovascular procedural treatments were deferred at scale during the COVID-19 pandemic, with unclear impact on patients presenting with non-ST-segment-elevation myocardial infarction (NSTEMI). Methods and Results In a retrospective cohort study of all patients diagnosed with NSTEMI in the US Veterans Affairs Healthcare System from January 1, 2019 to October 30, 2022 (n=67 125), procedural treatments and outcomes were compared between the prepandemic period and 6 unique pandemic phases: (1) acute phase, (2) community spread, (3) first peak, (4) post vaccine, (5) second peak, and (6) recovery. Multivariable regression analysis was performed to assess the association between pandemic phases and 30-day mortality. NSTEMI volumes dropped significantly with the pandemic onset (62.7% of prepandemic peak) and did not revert to prepandemic levels in subsequent phases, even after vaccine availability. Percutaneous coronary intervention and coronary artery bypass grafting volumes declined proportionally. Compared with the prepandemic period, patients with NSTEMI experienced higher 30-day mortality during Phases 2 and 3, even after adjustment for COVID-19-positive status, demographics, baseline comorbidities, and receipt of procedural treatment (adjusted odds ratio for Phases 2 and 3 combined, 1.26 [95% CI, 1.13-1.43], P<0.01). Patients receiving Veterans Affairs-paid community care had a higher adjusted risk of 30-day mortality compared with those at Veterans Affairs hospitals across all 6 pandemic phases. Conclusions Higher mortality after NSTEMI occurred during the initial spread and first peak of the pandemic but resolved before the second, higher peak-suggesting effective adaptation of care delivery but a costly delay to implementation. Investigation into the vulnerabilities of the early pandemic spread are vital to informing future resource-constrained practices.
Keywords: COVID‐19; acute coronary syndrome; acute myocardial infarction; non–ST‐segment–elevation myocardial infarction.
Figures
Similar articles
-
Effects of the COVID-19 pandemic on acute coronary syndromes in Germany during the first wave: the COVID-19 collateral damage study.Clin Res Cardiol. 2023 Apr;112(4):539-549. doi: 10.1007/s00392-022-02082-3. Epub 2022 Aug 17. Clin Res Cardiol. 2023. PMID: 35978111 Free PMC article.
-
Impact of the COVID-19 pandemic on time to treatment, treatment patterns and outcomes among patients with acute coronary syndrome in Yogyakarta, Indonesia: a retrospective cohort study.BMJ Open. 2024 Oct 14;14(10):e079060. doi: 10.1136/bmjopen-2023-079060. BMJ Open. 2024. PMID: 39401963 Free PMC article.
-
Case Rates, Treatment Approaches, and Outcomes in Acute Myocardial Infarction During the Coronavirus Disease 2019 Pandemic.JAMA Cardiol. 2020 Dec 1;5(12):1419-1424. doi: 10.1001/jamacardio.2020.3629. JAMA Cardiol. 2020. PMID: 32766756 Free PMC article.
-
Impact of COVID-19 Pandemic on the Outcomes of Acute Coronary Syndrome.Curr Probl Cardiol. 2023 Apr;48(4):101575. doi: 10.1016/j.cpcardiol.2022.101575. Epub 2022 Dec 27. Curr Probl Cardiol. 2023. PMID: 36584730 Free PMC article. Review.
-
Contemporary NSTEMI management: the role of the hospitalist.Hosp Pract (1995). 2020 Feb;48(1):1-11. doi: 10.1080/21548331.2020.1701329. Epub 2020 Feb 20. Hosp Pract (1995). 2020. PMID: 31815570 Review.
Cited by
-
Impact of the COVID-19 Pandemic on the Long-Term Prognosis of Acute Myocardial Infarction in Japan.Cureus. 2024 Jan 8;16(1):e51905. doi: 10.7759/cureus.51905. eCollection 2024 Jan. Cureus. 2024. PMID: 38333491 Free PMC article.
-
The impact of being in the COVID-19 pandemic on in-hospital mortality of non-infected patients aged 80 years and older with ST-elevation myocardial ınfarction.J Geriatr Cardiol. 2024 Jul 28;21(7):768-774. doi: 10.26599/1671-5411.2024.07.008. J Geriatr Cardiol. 2024. PMID: 39183956 Free PMC article. No abstract available.
-
Changes in the investigation and management of suspected myocardial infarction and injury during COVID-19: a multi-centre study using routinely collected healthcare data.Front Cardiovasc Med. 2024 May 21;11:1406608. doi: 10.3389/fcvm.2024.1406608. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38836064 Free PMC article.
References
-
- Veterans Health Administration–Office of Emergency Management . COVID‐19 Response Plan. Accessed June 2, 2020. https://www.va.gov/opa/docs/VHA_COVID_19_03232020_vF_1.pdf.
-
- Centers for Disease Control and Prevention . Managing Healthcare Operations during COVID‐19. Accessed January 12, 2022. https://www.cdc.gov/coronavirus/2019‐ncov/healthcare‐facilities/guidance....
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE Jr, Ganiats TG, Holmes DR Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, et al. 2014 AHA/ACC guideline for the management of patients with non–ST‐elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:344–426. doi: 10.1161/CIR.0000000000000134 - DOI
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, et al. 2013 ACCF/AHA guideline for the management of ST‐elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:362–425. doi: 10.1161/CIR.0b013e3182742c84 - DOI - PubMed
-
- Mohamed MO, Banerjee A, Clarke S, de Belder M, Patwala A, Goodwin AT, Kwok CS, Rashid M, Gale CP, Curzen N, et al. Impact of COVID‐19 on cardiac procedure activity in England and associated 30‐day mortality. Eur Heart J Qual Care Clin Outcomes. 2021;7:247–256. doi: 10.1093/ehjqcco/qcaa079 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
