

Impact of gas humidification and nebulizer position under invasive ventilation: preclinical comparative study of regional aerosol deposition
- PMID: 37422519
- PMCID: PMC10329710
- DOI: 10.1038/s41598-023-38281-9
Impact of gas humidification and nebulizer position under invasive ventilation: preclinical comparative study of regional aerosol deposition
Abstract
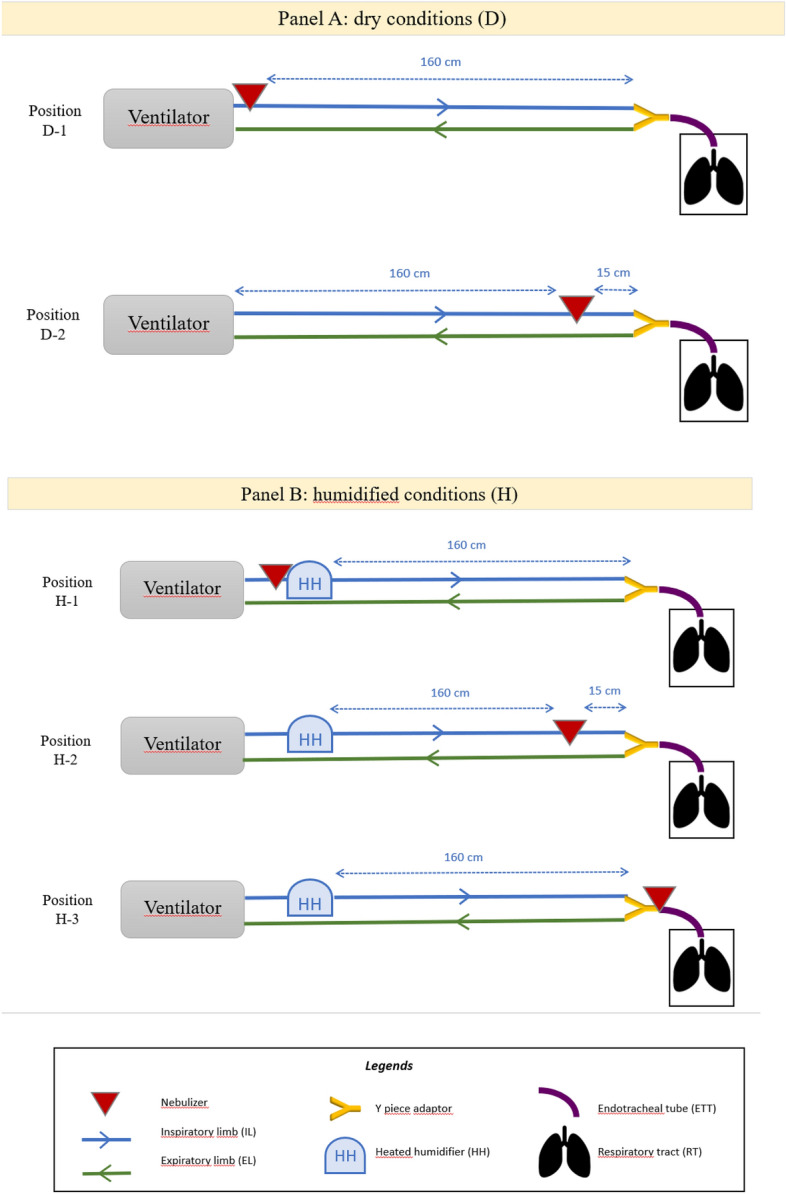
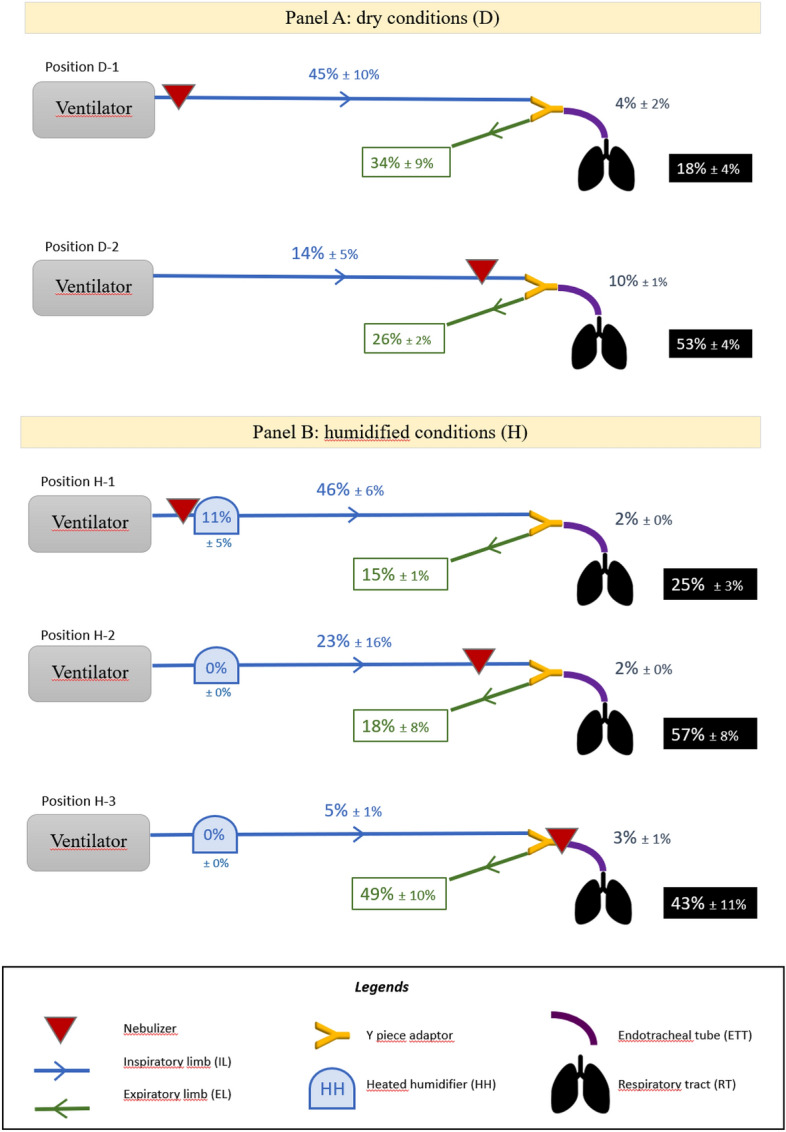
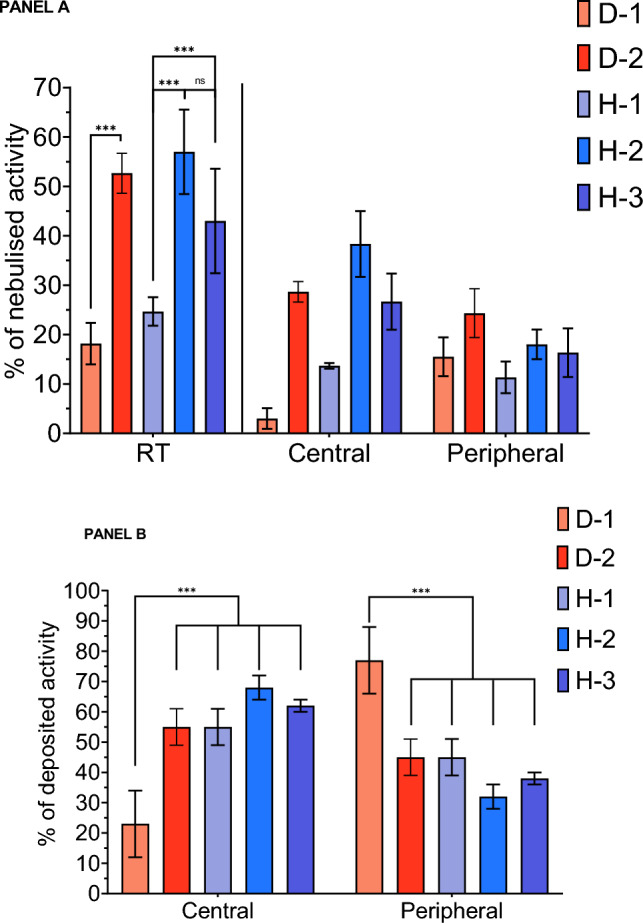
Successful aerosol therapy in mechanically ventilated patients depends on multiple factors. Among these, position of nebulizer in ventilator circuit and humidification of inhaled gases can strongly influence the amount of drug deposited in airways. Indeed, the main objective was to preclinically evaluate impact of gas humidification and nebulizer position during invasive mechanical ventilation on whole lung and regional aerosol deposition and losses. Ex vivo porcine respiratory tracts were ventilated in controlled volumetric mode. Two conditions of relative humidity and temperature of inhaled gases were investigated. For each condition, four different positions of vibrating mesh nebulizer were studied: (i) next to the ventilator, (ii) right before humidifier, (iii) 15 cm to the Y-piece adapter and (iv) right after the Y-piece. Aerosol size distribution were calculated using cascade impactor. Nebulized dose, lung regional deposition and losses were assessed by scintigraphy using 99mtechnetium-labeled diethylene-triamine-penta-acetic acid. Mean nebulized dose was 95% ± 6%. For dry conditions, the mean respiratory tract deposited fractions reached 18% (± 4%) next to ventilator and 53% (± 4%) for proximal position. For humidified conditions, it reached 25% (± 3%) prior humidifier, 57% (± 8%) before Y-piece and 43% (± 11%) after this latter. Optimal nebulizer position is proximal before the Y-piece adapter showing a more than two-fold higher lung dose than positions next to the ventilator. Dry conditions are more likely to cause peripheral deposition of aerosols in the lungs. But gas humidification appears hard to interrupt efficiently and safely in clinical use. Considering the impact of optimized positioning, this study argues to maintain humidification.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Effect of Interrupting Heated Humidification on Nebulized Drug Delivery Efficiency, Temperature, and Absolute Humidity During Mechanical Ventilation: A Multi-Lab In Vitro Study.J Aerosol Med Pulm Drug Deliv. 2024 Jun;37(3):115-124. doi: 10.1089/jamp.2023.0028. Epub 2024 Apr 2. J Aerosol Med Pulm Drug Deliv. 2024. PMID: 38563793
-
Influence of nebulizer type, position, and bias flow on aerosol drug delivery in simulated pediatric and adult lung models during mechanical ventilation.Respir Care. 2010 Jul;55(7):845-51. Respir Care. 2010. PMID: 20587095
-
In-Vitro Comparison of Single Limb and Dual Limb Circuit for Aerosol Delivery via Noninvasive Ventilation.Respir Care. 2022 Jul;67(7):807-813. doi: 10.4187/respcare.09543. Epub 2022 Apr 26. Respir Care. 2022. PMID: 35473786
-
Not all nebulizers are created equal: Considerations in choosing a nebulizer for aerosol delivery during mechanical ventilation.Expert Rev Respir Med. 2023 Feb;17(2):131-142. doi: 10.1080/17476348.2023.2183194. Epub 2023 Feb 27. Expert Rev Respir Med. 2023. PMID: 36803134 Review.
-
Inhaled bronchodilator administration during mechanical ventilation.Respir Care. 2004 Jun;49(6):623-34. Respir Care. 2004. PMID: 15165297 Review.
Cited by
-
Towards More Precise Targeting of Inhaled Aerosols to Different Areas of the Respiratory System.Pharmaceutics. 2024 Jan 10;16(1):97. doi: 10.3390/pharmaceutics16010097. Pharmaceutics. 2024. PMID: 38258107 Free PMC article. Review.
-
An in vitro study of the effects of respiratory circuit setup and parameters on aerosol delivery during mechanical ventilation.Front Med (Lausanne). 2024 Jan 24;10:1307301. doi: 10.3389/fmed.2023.1307301. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38327274 Free PMC article.
References
-
- Ehrmann S, Roche-Campo F, Bodet-Contentin L, Razazi K, Dugernier J, Trenado-Alvarez J, Donzeau A, Vermeulen F, Thévoz D, Papanikolaou M, Edelson A, León Yoshido H, Piquilloud L, Lakhal K, Lopes C, Vicent C, Desachy A, Apiou-Sbirlea G, Isabey D, Brochard L. Reva Research Network, AT@ICU Study Group, Aerosol therapy in intensive and intermediate care units: Prospective observation of 2808 critically ill patients. Intensive Care Med. 2016;42:192–201. doi: 10.1007/s00134-015-4114-5. - DOI - PubMed
-
- Dhand R. Special problems in aerosol delivery: Artificial airways. Respir. Care. 2000;45:636–645. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
