

Efficacy and safety of adjunctive corticosteroids in the treatment of severe community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials
- PMID: 37422686
- PMCID: PMC10329791
- DOI: 10.1186/s13054-023-04561-z
Efficacy and safety of adjunctive corticosteroids in the treatment of severe community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials
Erratum in
-
Correction to: Efficacy and safety of adjunctive corticosteroids in the treatment of severe community‑acquired pneumonia: a systematic review and meta‑analysis of randomized controlled trials.Crit Care. 2023 Oct 27;27(1):411. doi: 10.1186/s13054-023-04710-4. Crit Care. 2023. PMID: 37891660 Free PMC article. No abstract available.
Abstract
Background: This systematic review and meta-analysis aimed to investigate the clinical efficacy and safety of systemic corticosteroids in the treatment of patients with severe community-acquired pneumonia (sCAP).
Methods: A comprehensive search was conducted using the Medline, Embase, ClinicalTrials.gov, and Scopus databases for articles published until April 24, 2023. Only randomized controlled trials (RCTs) that assessed the clinical efficacy and safety of adjunctive corticosteroids for treating sCAP were included. The primary outcome was the 30-day all-cause mortality.
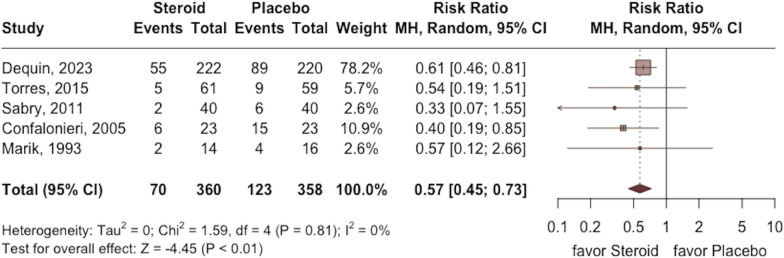
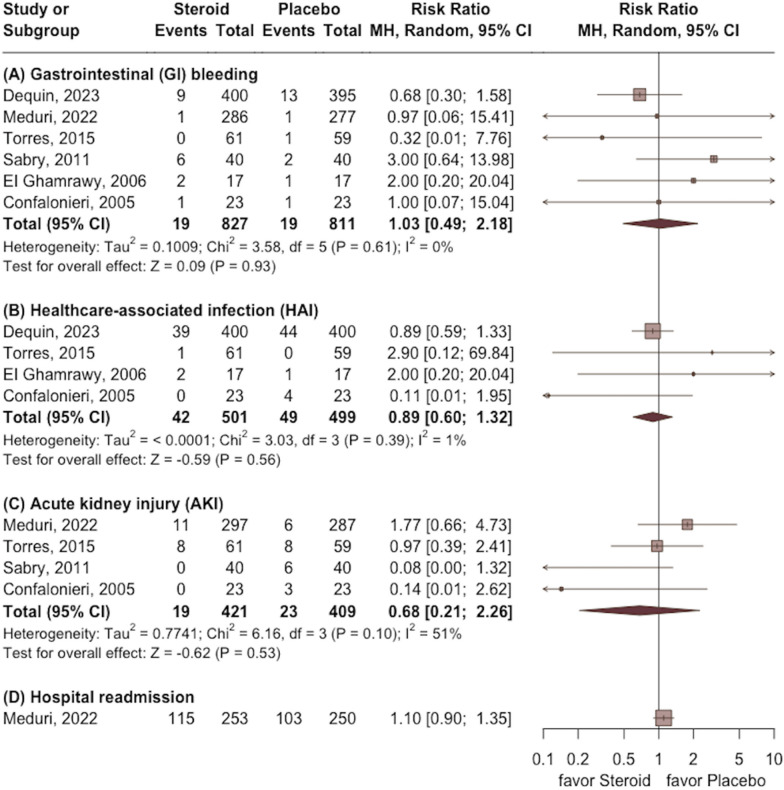
Results: A total of severe RCTs involving 1689 patients were included in this study. Overall, the study group had a lower mortality rate at day 30 than the control group (risk ratio [RR], 0.61; 95% CI 0.44 to 0.85; p < 0.01) with low heterogeneity (I2 = 0%, p = 0.42). Compared to the control group, the study group had a lower risk of the requirement of mechanical ventilation (RR 0.57; 95% CI 0.45 to 0.73; p < 0.001), shorter length of intensive care unit (MD - 0.8; 95% CI - 1.4 to - 0.1; p = 0.02), and hospital stay (MD - 1.1; 95% CI - 2.0 to - 0.1; p = 0.04). Finally, no significant difference was observed between the study and the control groups in terms of gastrointestinal tract bleeding (RR 1.03; 95% CI 0.49 to 2.18; p = 0.93), healthcare-associated infection (RR 0.89; 95% CI 0.60 to 1.32; p = 0.56), and acute kidney injury (RR 0.68; 95% CI 0.21 to 2.26; p = 0.53).
Conclusions: In patients with sCAP, adjunctive corticosteroids can provide survival benefits and improve clinical outcomes without increasing adverse events. However, because the pooled evidence remains inconclusive, further studies are required.
Keywords: Community-acquired pneumonia; Corticosteroid; Hydrocortisone; Intensive care unit; Mortality.
© 2023. The Author(s).
Conflict of interest statement
All authors declare that there was no conflict of interest.
Figures




Comment in
-
Letter to the Editor Regarding "Efficacy and safety of adjunctive corticosteroids in the treatment of severe community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials".Crit Care. 2023 Jul 24;27(1):296. doi: 10.1186/s13054-023-04576-6. Crit Care. 2023. PMID: 37488594 Free PMC article. No abstract available.
-
Effects of corticosteroids on severe community-acquired pneumonia: a closer look at the evidence.Crit Care. 2023 Aug 29;27(1):336. doi: 10.1186/s13054-023-04614-3. Crit Care. 2023. PMID: 37644607 Free PMC article. No abstract available.
-
Final approval for corticosteroids in severe CAP? For sure, in septic shock.Crit Care. 2023 Sep 4;27(1):342. doi: 10.1186/s13054-023-04613-4. Crit Care. 2023. PMID: 37667250 Free PMC article. No abstract available.
-
Comments on "Efficacy and safety of adjunctive corticosteroids in the treatment of severe community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials".Crit Care. 2023 Sep 6;27(1):348. doi: 10.1186/s13054-023-04619-y. Crit Care. 2023. PMID: 37674233 Free PMC article. No abstract available.
-
Effect of corticosteroids on mortality in patients with community-acquired pneumonia.Crit Care. 2023 Sep 19;27(1):358. doi: 10.1186/s13054-023-04645-w. Crit Care. 2023. PMID: 37726854 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
