

Defining the clinical validity of genes reported to cause pulmonary arterial hypertension
- PMID: 37422716
- PMCID: PMC10766870
- DOI: 10.1016/j.gim.2023.100925
Defining the clinical validity of genes reported to cause pulmonary arterial hypertension
Abstract
Purpose: Pulmonary arterial hypertension (PAH) is a rare, progressive vasculopathy with significant cardiopulmonary morbidity and mortality. Genetic testing is currently recommended for adults diagnosed with heritable, idiopathic, anorexigen-, hereditary hemorrhagic telangiectasia-, and congenital heart disease-associated PAH, PAH with overt features of venous/capillary involvement, and all children diagnosed with PAH. Variants in at least 27 genes have putative evidence for PAH causality. Rigorous assessment of the evidence is needed to inform genetic testing.
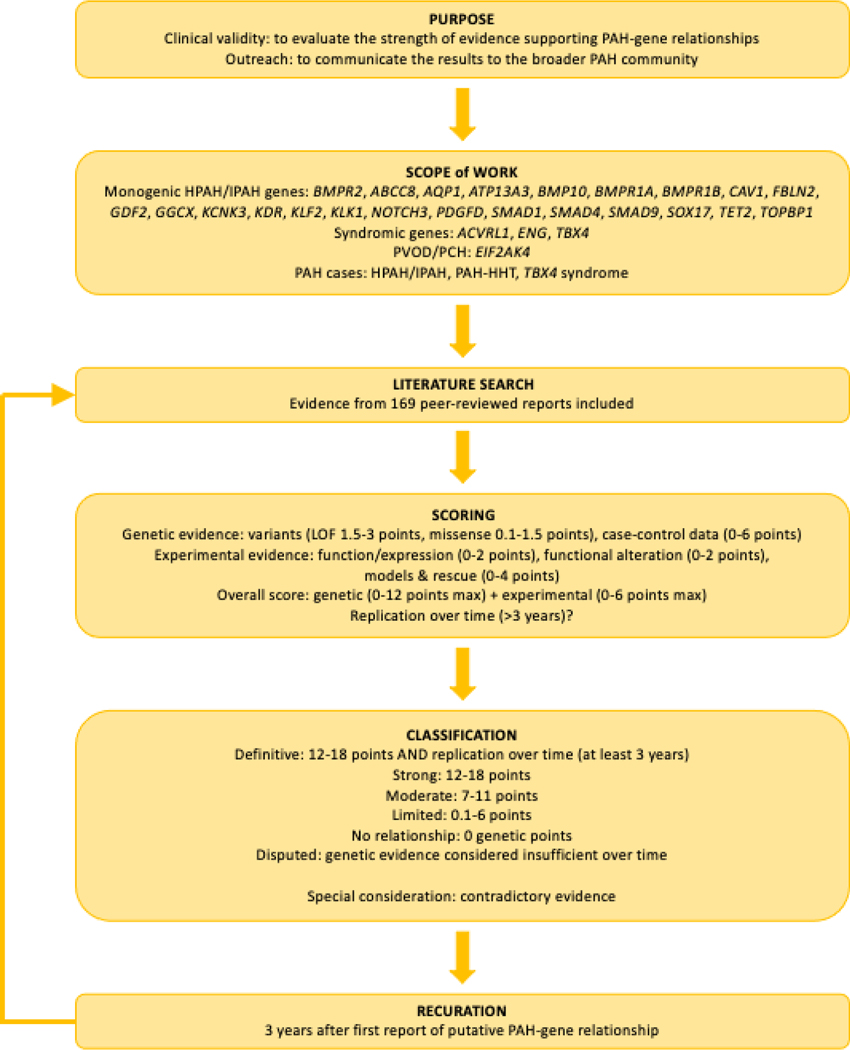
Methods: An international panel of experts in PAH applied a semi-quantitative scoring system developed by the NIH Clinical Genome Resource to classify the relative strength of evidence supporting PAH gene-disease relationships based on genetic and experimental evidence.
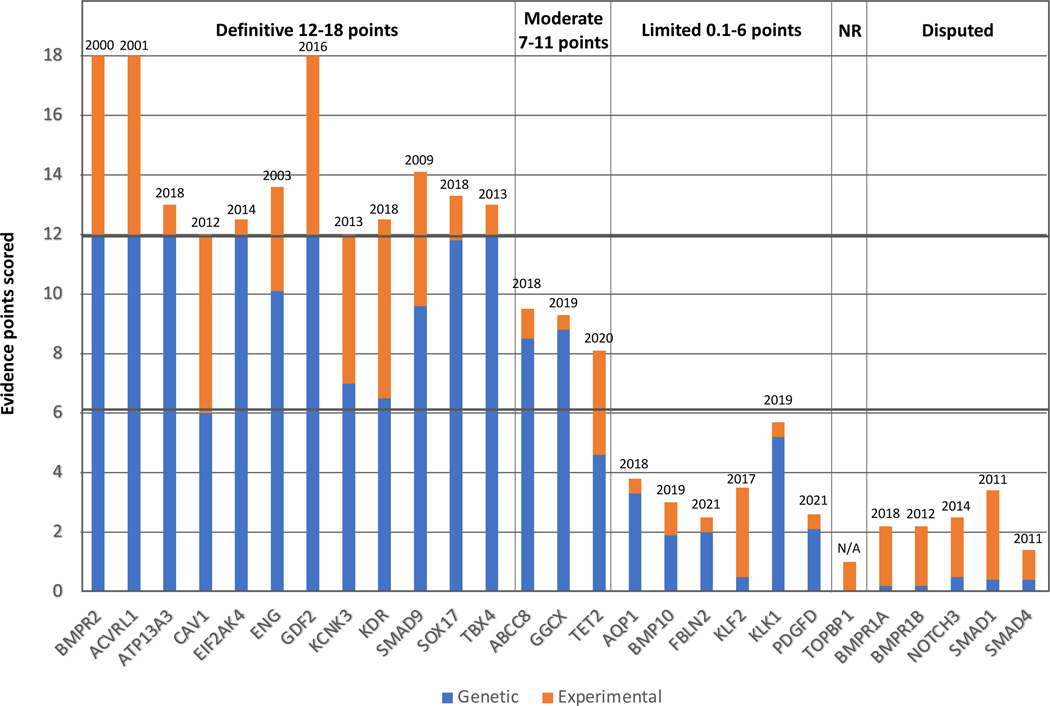
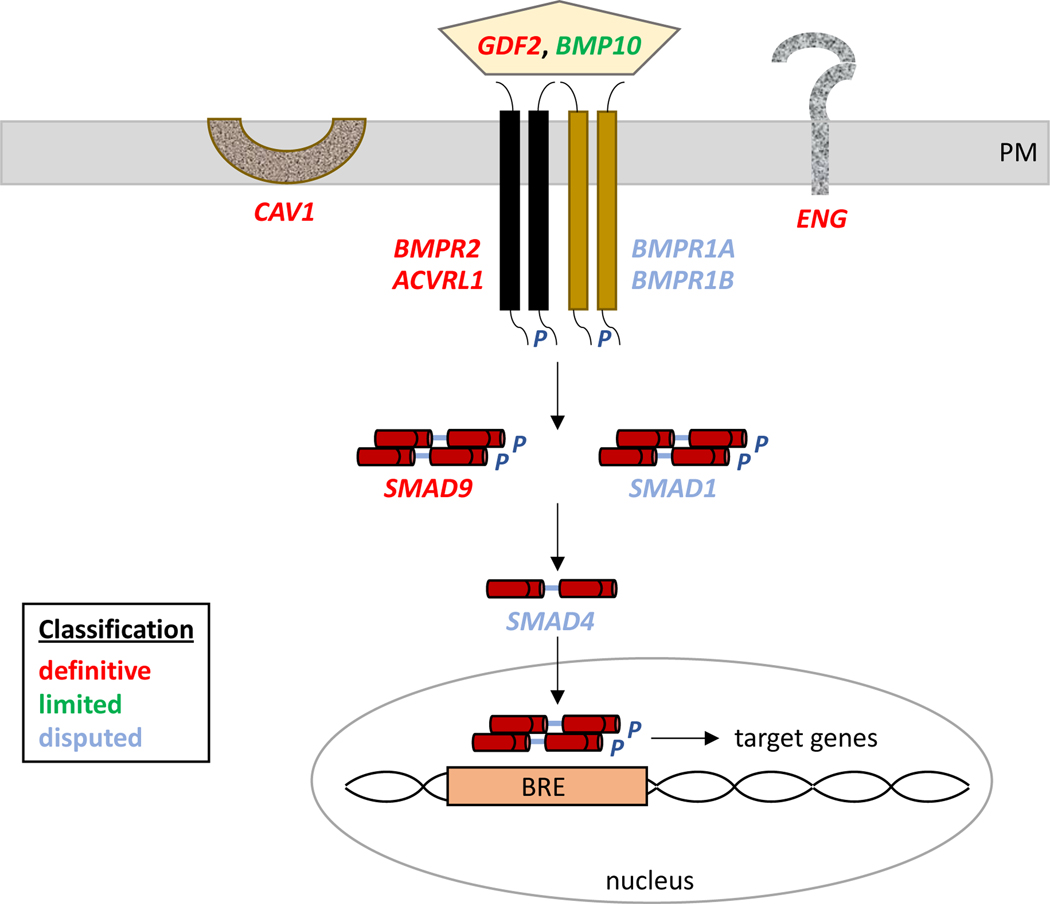
Results: Twelve genes (BMPR2, ACVRL1, ATP13A3, CAV1, EIF2AK4, ENG, GDF2, KCNK3, KDR, SMAD9, SOX17, and TBX4) were classified as having definitive evidence and 3 genes (ABCC8, GGCX, and TET2) with moderate evidence. Six genes (AQP1, BMP10, FBLN2, KLF2, KLK1, and PDGFD) were classified as having limited evidence for causal effects of variants. TOPBP1 was classified as having no known PAH relationship. Five genes (BMPR1A, BMPR1B, NOTCH3, SMAD1, and SMAD4) were disputed because of a paucity of genetic evidence over time.
Conclusion: We recommend that genetic testing includes all genes with definitive evidence and that caution be taken in the interpretation of variants identified in genes with moderate or limited evidence. Genes with no known evidence for PAH or disputed genes should not be included in genetic testing.
Keywords: Genetics; Genomic medicine; Molecular diagnosis; Pulmonary arterial hypertension.
Copyright © 2023 American College of Medical Genetics and Genomics. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest The authors declare no conflicts of interest.
Figures
References
-
- Vonk-Noordegraaf A, Haddad F, Chin KM, et al. Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. J Am Coll Cardiol 2013: 62(25 Suppl): D22–33. - PubMed
-
- Galie N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Rev Esp Cardiol (Engl Ed) 2016: 69(2): 177. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
