

Inferior vena cava distensibility from subcostal and trans-hepatic imaging using both M-mode or artificial intelligence: a prospective study on mechanically ventilated patients
- PMID: 37423948
- PMCID: PMC10329966
- DOI: 10.1186/s40635-023-00529-z
Inferior vena cava distensibility from subcostal and trans-hepatic imaging using both M-mode or artificial intelligence: a prospective study on mechanically ventilated patients
Abstract
Background: Variation of inferior vena cava (IVC) is used to predict fluid-responsiveness, but the IVC visualization with standard sagittal approach (SC, subcostal) cannot be always achieved. In such cases, coronal trans-hepatic (TH) window may offer an alternative, but the interchangeability of IVC measurements in SC and TH is not fully established. Furthermore, artificial intelligence (AI) with automated border detection may be of clinical value but it needs validation.
Methods: Prospective observational validation study in mechanically ventilated patients with pressure-controlled mode. Primary outcome was the IVC distensibility (IVC-DI) in SC and TH imaging, with measurements taken both in M-Mode or with AI software. We calculated mean bias, limits of agreement (LoA), and intra-class correlation (ICC) coefficient.
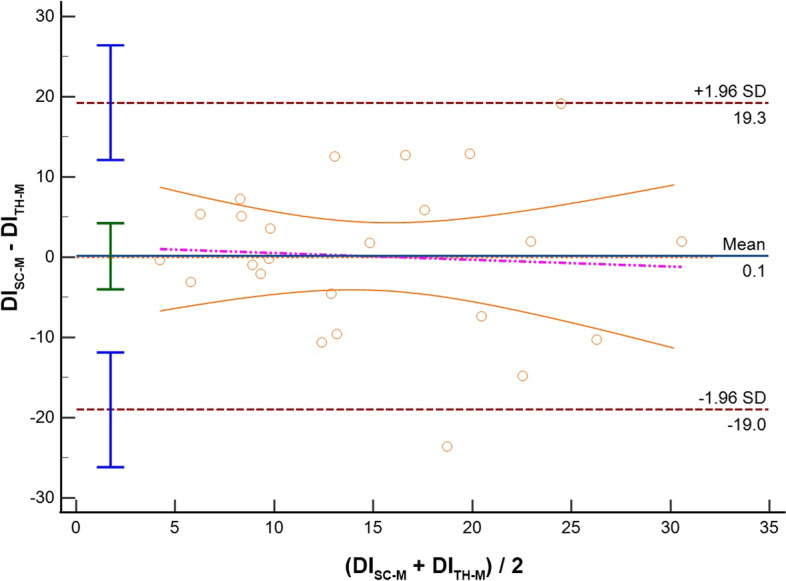
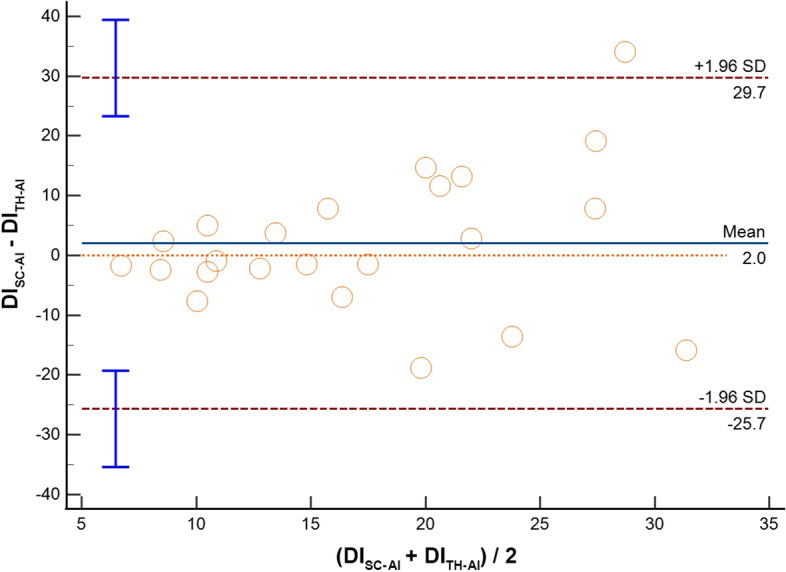
Results: Thirty-three patients were included. Feasibility rate was 87.9% and 81.8% for SC and TH visualization, respectively. Comparing imaging from the same anatomical site acquired with different modalities (M-Mode vs AI), we found the following IVC-DI differences: (1) SC: mean bias - 3.1%, LoA [- 20.1; 13.9], ICC = 0.65; (2) TH: mean bias - 2.0%, LoA [- 19.3; 15.4], ICC = 0.65. When comparing the results obtained from the same modality but from different sites (SC vs TH), IVC-DI differences were: (3) M-Mode: mean bias 1.1%, LoA [- 6.9; 9.1], ICC = 0.54; (4) AI: mean bias 2.0%, LoA [- 25.7; 29.7], ICC = 0.32.
Conclusions: In patients mechanically ventilated, AI software shows good accuracy (modest overestimation) and moderate correlation as compared to M-mode assessment of IVC-DI, both for SC and TH windows. However, precision seems suboptimal with wide LoA. The comparison of M-Mode or AI between different sites yields similar results but with weaker correlation. Trial registration Reference protocol: 53/2022/PO, approved on 21/03/2022.
Keywords: Critical care; Inferior vena cava; Subcostal; Transhepatic; Ultrasound.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no conflict of interests.
Figures


References
-
- Sanfilippo F, Scolletta S (2017) Fluids in cardiac surgery: sailing calm on a stormy sea? Common sense is the guidance. Minerva anestesiologica - PubMed
LinkOut - more resources
Full Text Sources
