Does Post-traumatic Stress Disorder Impact Treatment Outcomes within a Randomised Controlled Trial of Mitochondrial Agents for Bipolar Depression?
- PMID: 37424414
- PMCID: PMC10335917
- DOI: 10.9758/cpn.22.981
Does Post-traumatic Stress Disorder Impact Treatment Outcomes within a Randomised Controlled Trial of Mitochondrial Agents for Bipolar Depression?
Abstract
Objective: Bipolar disorder often co-occurs with post-traumatic stress disorder, yet few studies have investigated the impact of post-traumatic stress disorder in bipolar disorder on treatment outcomes. The aim of this sub-analysis was to explore symptoms and functioning outcomes between those with bipolar disorder alone and those with comorbid bipolar disorder and post-traumatic stress disorder.
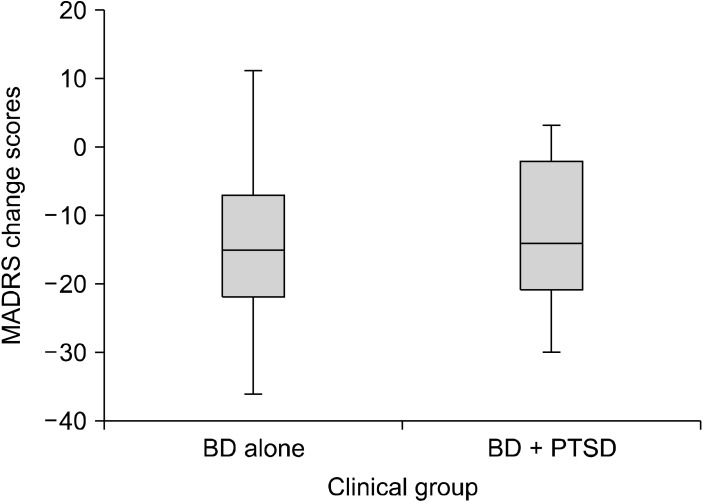
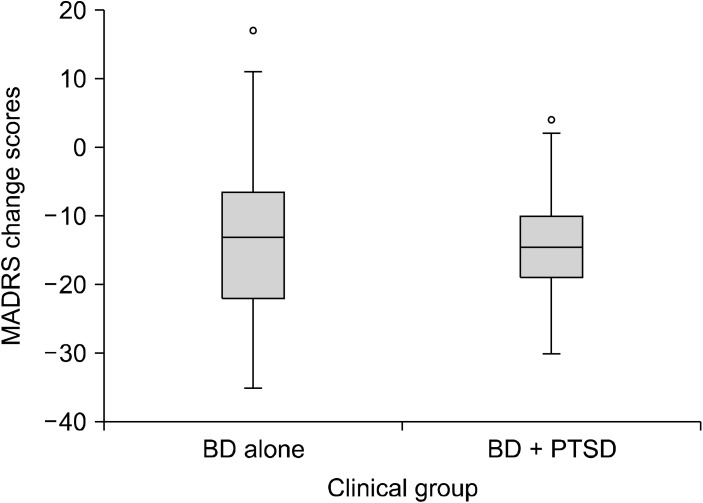
Methods: Participants (n = 148) with bipolar depression were randomised to: (i) N-acetylcysteine alone; (ii) a combination of nutraceuticals; (iii) or placebo (in addition to treatment as usual) for 16 weeks (+4 weeks discontinuation). Differences between bipolar disorder and comorbid bipolar disorder and post-traumatic stress disorder on symptoms and functioning at five timepoints, as well as on the rate of change from baseline to week 16 and baseline to week 20, were examined.
Results: There were no baseline differences between bipolar disorder alone and comorbid bipolar disorder and post-traumatic stress disorder apart from the bipolar disorder alone group being significantly more likely to be married (p = 0.01). There were also no significant differences between bipolar disorder alone and comorbid bipolar disorder and post-traumatic stress disorder on symptoms and functioning.
Conclusion: There were no differences in clinical outcomes over time within the context of an adjunctive randomised controlled trial between those with bipolar disorder alone compared to those with comorbid bipolar disorder and post-traumatic stress disorder. However, differences in psychosocial factors may provide targets for areas of specific support for people with comorbid bipolar disorder and post-traumatic stress disorder.
Keywords: Bipolar disorder; Comorbidity; Depression; Psychiatry; Stress disorders; post-traumatic.
Conflict of interest statement
SER has received grant/research support from Deakin University. ALW has received grant/research support from Deakin University. and the Rotary Club of Geelong. OMD is a R.D. Wright Biomedical NHMRC Career Development Fellow (APP1145634) and has received grant support from the Brain and Behavior Foundation, Simons Autism Foundation, Stanley Medical Research Institute, Deakin University, Lilly, NHMRC and ASBDD/Servier. She has also received in kind support from BioMedica Nutracuticals, NutritionCare and Bioceuticals. MMA has received grant/ research support from Deakin University, Australasian Society for Bipolar Depressive Disorders, Lundbeck, Australian Rotary Health, Ian Parker Bipolar Research Fund and Cooperative Research Centre for Mental Health and PDG Geoff and Betty Betts Award from Rotary Club of Geelong. MB has received grant/research support from the NIH, Cooperative Research Centre, Simons Autism Foundation, Cancer Council of Victoria, Stanley Medical Research Foundation, Medical Benefits Fund, National Health and Medical Research Council, Medical Research Futures Fund, Beyond Blue, Rotary Health, A2 milk company, Meat and Livestock Board, Woolworths, Avant and the Harry Windsor Foundation, has been a speaker for Astra Zeneca, Lundbeck, Merck, Pfizer, and served as a consultant to Allergan, Astra Zeneca, Bioadvantex, Bionomics, Collaborative Medicinal Development, Lundbeck Merck, Pfizer and Servier. SC is a NHMRC Senior Research Fellow (APP1136344) and has received money from NHRMC, Wellcome Trust, and HCF Research Foundation. AT has received travel or grant support from NHMRC, AMP Foundation, Stroke Foundation, Hunter Medical Research Institute, Helen Macpherson Smith Trust, Schizophrenia Fellowship NSW, SMHR, ISAD, the University of Newcastle and Deakin University. MM has received Grant/research support from NHMRC, Deakin University School of Medicine, Deakin Biostatistics Unit, Institute for Mental and Physical Health and Clinical Translation, and Medibank Health Research Fund. SD has received Grant/Research Support from the Stanley Medical Research Institute, NHMRC, Beyond Blue, ARHRF, Simons Foundation, Geelong Medical Research Foundation, Fondation FondaMental, Eli Lilly, GlaxoSmithKline, Organon, Mayne Pharma and Servier, speaker's fees from Eli Lilly, advisory board fees from Eli Lilly and Novartis and conference travel support from Servier. GM has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, Ramsay Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca and Servier; has been a speaker for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen Cilag, Lundbeck, Otsuka and Servier. CN had served in the Servier, Janssen-Cilag, Wyeth and Eli Lilly Advisory Boards, received research grant support from Wyeth and Lundbeck, and honoraria from Servier, Bristol-Myers Squibb, Organon, Eli Lilly, GlaxoSmithKline, Janssen- Cilag, Astra-Zenaca, Wyeth, and Pfizer.
Figures
References
-
- Australian Bureau of Statistics, author. Catalogue No. 4236.0. National Survey of Mental Health and Wellbeing: Summary of results. Australian Bureau of Statistics; Canberra: 2008.
-
- Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:617–627. doi: 10.1001/archpsyc.62.6.617. Erratum in: Arch Gen Psychiatry 2005;62:709. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources