

doi: 10.1016/j.eats.2023.02.008.
eCollection 2023 Jun.
An All-Arthroscopic Simple Double 360° Lasso Loop Technique for Supraopectoral Biceps Tenodesis
Affiliations
- PMID: 37424650
- PMCID: PMC10323638
- DOI: 10.1016/j.eats.2023.02.008
Item in Clipboard
An All-Arthroscopic Simple Double 360° Lasso Loop Technique for Supraopectoral Biceps Tenodesis
Arthrosc Tech.
.
Abstract
In many shoulder joint diseases, there is often a combination of long head biceps tendon(LHBT)pathology. Biceps pathology is one of the main causes of shoulder pain, and it is effectively managed with tenodesis. Biceps tenodesis can be performed in a variety of ways with different fixation and at different locations. This article introduces an all-arthroscopic suprapectoral biceps tenodesis technique with a 2-suture anchor. Double 360° Lasso Loop is used to fix the biceps tendon, and only one puncture of the biceps tendon was required, which caused little damage to the tendon and was not easy for the suture to slip and fail.
© 2023 The Authors.
Figures

Location of arthroscopic portals (right shoulder). Suprapectoral biceps portal is at the level of the apex of the axillary fold (red arrow).
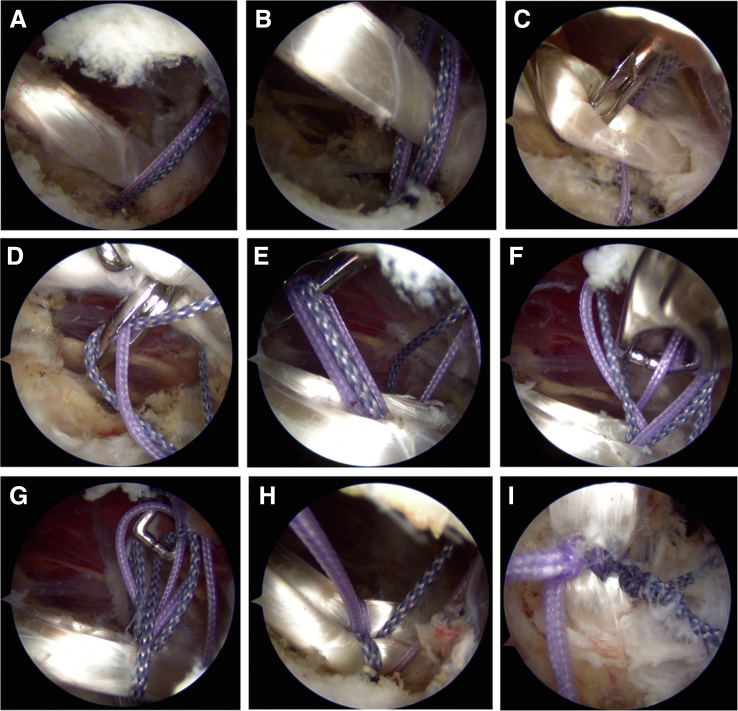
(A-I) Patient’s right shoulder positioned in the lateral decubitus and viewing through a lateral portal. (A) Through the suprapectoral-biceps portal a 4.5-mm 2-suture anchor (Depuy, Healix) is placed at the upper margin of the pectoralis major and slightly posterior to the bicipital groove through the suprapectoral biceps portal. (B) The different strands of the two sutures are placed on each side of the biceps tendon with a probe or suture grasper (Smith & Nephew) from the suprapectoral-biceps portal. (C) From the suprapectoral-biceps portal a penetrating grasper (Smith & Nephew) is used to puncture the biceps tendon near the proximal position above the anchor. (D) After the tip of the penetrating grasper passed through the midportion of the biceps tendon, one of the two sutures on each side of LHBT with different colors is retrieved by using the jaw of the penetrating suture grasper (Smith & Nephew), respectively. (E) Pull out the captured two sutures, but not completely through, leaving two loops of suture exiting the superior surface of the tendon. (F) A suture grasper (Smith & Nephew) is passed through the two loops from the anterolateral portal to grasp the free end of the suture in front of the biceps tendon, which is the same suture limb used to create the loops. The suture limb is pulled through the double loops. (G) Repeated the same procedure from the front of the double loops to grasp another free limb of the suture behind the biceps tendon through the suprapectoral-biceps portal, which is another strand used to create the loops. (H) The ends of all four sutures are tightened. (I) After two nonsliding knots are tied on both side of the biceps tendon, the double 360° lasso loop configuration is achieved.
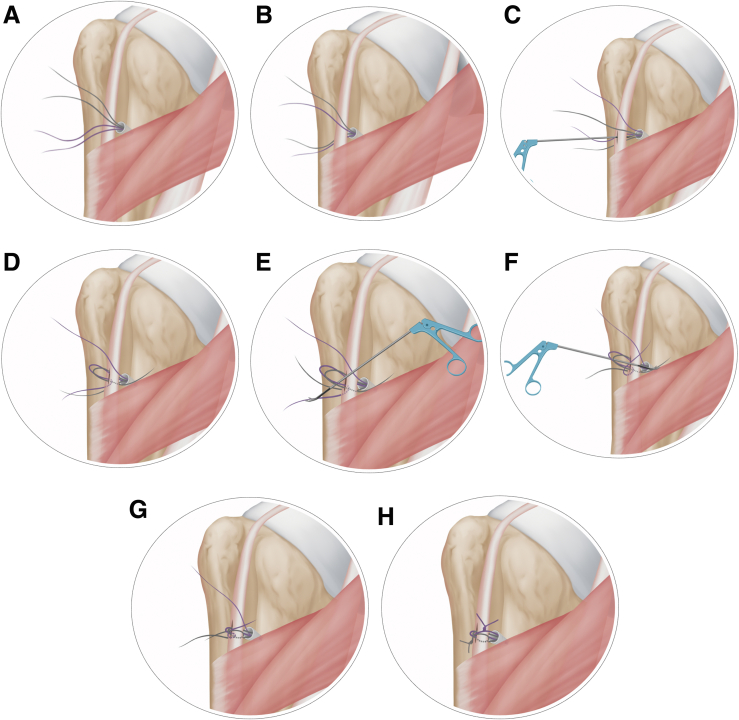
(A-H) Illustrations summarizing the steps required to create the double 360° lasso loop. (A) A 4.5-mm 2-suture anchor is placed at the upper margin of the pectoralis major and near the bicipital groove. (B) The different strands of the two sutures are placed on each side of the biceps tendon. (C) A penetrating grasper is used to puncture the biceps tendon near the proximal position above the anchor. (D) One of the two sutures on each side of LHBT with different colors is retrieved by using the jaw of the penetrating suture grasper, respectively. And leaving two suture loops above the surface of the tendon. (E) A suture grasper is passed through the two loops from the front of the double loops to grasp the free end of the suture behind the biceps tendon, which is the same suture limb used to create the loops. The suture limb is pulled through the double loops. (F) The same procedure is done from the rear of the biceps tendon to grasp another free limb of the suture in front of the biceps tendon, which is another strand used to create the loops. (G) The ends of all four sutures are tightened. (H) Tied two nonsliding knots on both sides of the biceps tendon, the double 360° lasso loop is finished.
Similar articles
-
A Simple, All-Arthroscopic, Knotless Suture Lasso Loop Technique for Suprapectoral Biceps Tenodesis.Arthrosc Tech. 2017 May 22;6(3):e635-e639. doi: 10.1016/j.eats.2017.01.008. eCollection 2017 Jun. Arthrosc Tech. 2017. PMID: 28706810 Free PMC article.
-
Arthroscopic extra-articular suprapectoral biceps tenodesis with knotless suture anchor.Eur J Orthop Surg Traumatol. 2019 Feb;29(2):493-497. doi: 10.1007/s00590-018-2301-0. Epub 2018 Aug 25. Eur J Orthop Surg Traumatol. 2019. PMID: 30145670
-
Surgical technique for arthroscopic onlay suprapectoral biceps tenodesis with an all-suture anchor.JSES Open Access. 2018 Mar 13;2(1):69-73. doi: 10.1016/j.jses.2017.12.001. eCollection 2018 Mar. JSES Open Access. 2018. PMID: 30675570 Free PMC article.
-
Outcomes and Complications After Primary Arthroscopic Suprapectoral Versus Open Subpectoral Biceps Tenodesis for Superior Labral Anterior-Posterior Tears or Biceps Abnormalities: A Systematic Review and Meta-analysis.Orthop J Sports Med. 2020 Aug 28;8(8):2325967120945322. doi: 10.1177/2325967120945322. eCollection 2020 Aug. Orthop J Sports Med. 2020. PMID: 32923502 Free PMC article. Review.
-
Suture anchor and percutaneous intra-articular transtendon biceps tenodesis.Sports Med Arthrosc Rev. 2008 Sep;16(3):177-9. doi: 10.1097/JSA.0b013e3181824efd. Sports Med Arthrosc Rev. 2008. PMID: 18703978 Review.
References
-
- Elser F., Braun S., Dewing C.B., Giphart J.E., Millett P.J. Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon. Arthroscopy. 2011;27:581–592. - PubMed
-
- Koh K.H., Ahn J.H., Kim S.M., Yoo J.C. Treatment of biceps tendon lesions in the setting of rotator cuff tears: Prospective cohort study of tenotomy versus tenodesis. Am J Sports Med. 2010;38:1584–1590. - PubMed
-
- Griffin J.W., Cvetanovich G.L., Kim J., et al. Biceps tenodesis is a viable option for management of proximal biceps injuries in patients less than 25 years of age. Arthroscopy. 2019;35:1036–1041. - PubMed
-
- Gurnani N., van Deurzen D.F., Janmaat V.T., van den Bekerom M.P. Tenotomy or tenodesis for pathology of the long head of the biceps brachii: A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2016;24:3765–3771. - PubMed
-
- de Sa D., Arakgi M.E., Lian J., Crum R.J., Lin A., Lesniak B.P. Labral repair versus biceps tenodesis for primary surgical management of type II superior labrum anterior to posterior tears: A systematic review. Arthroscopy. 2019;35:1927–1938. - PubMed
LinkOut - more resources
Full Text Sources
