

Cost-effectiveness of expanded antiviral treatment for chronic hepatitis B virus infection in China: an economic evaluation
- PMID: 37424693
- PMCID: PMC10326688
- DOI: 10.1016/j.lanwpc.2023.100738
Cost-effectiveness of expanded antiviral treatment for chronic hepatitis B virus infection in China: an economic evaluation
Abstract
Background: China, which has the largest chronic hepatitis B virus (HBV) burden, may expand antiviral therapy to attain the World Health Organization (WHO)-2030 goal of 65% reduction in mortality. We evaluated health outcomes and cost-effectiveness of chronic HBV infection treatments based on alanine transaminase (ALT) antiviral treatment initiation thresholds and coverage in China to identify an optimal strategy.
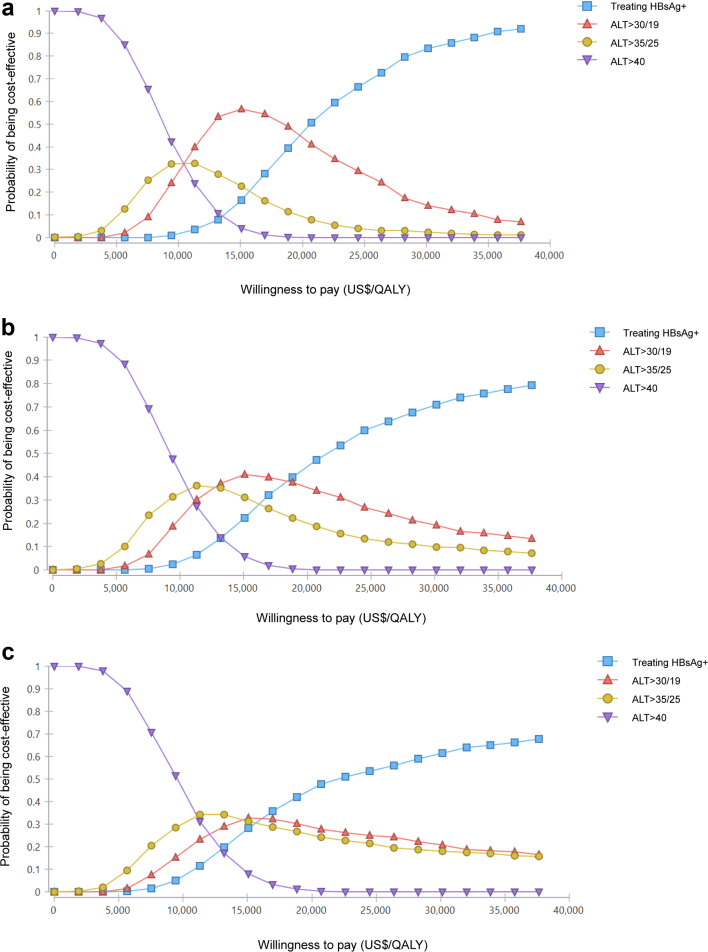
Methods: A decision-tree Markov state-transition model evaluated the cost-effectiveness of expanded antiviral treatment for chronic HBV infection by simulating 136 scenarios by ALT treatment initiation thresholds (40 U/L, 35 U/L for males and 25 U/L for females, 30 U/L for males and 19 U/L for females, and treating HBsAg+ individuals regardless of ALT values), population age groups (18-80, 30-80, and 40-80 years), implementation durations (2023, 2028, and 2033) under and treatment coverages (20%, 40%, 60%, and 80%). Deterministic and probabilistic sensitivity analyses explored model uncertainty.
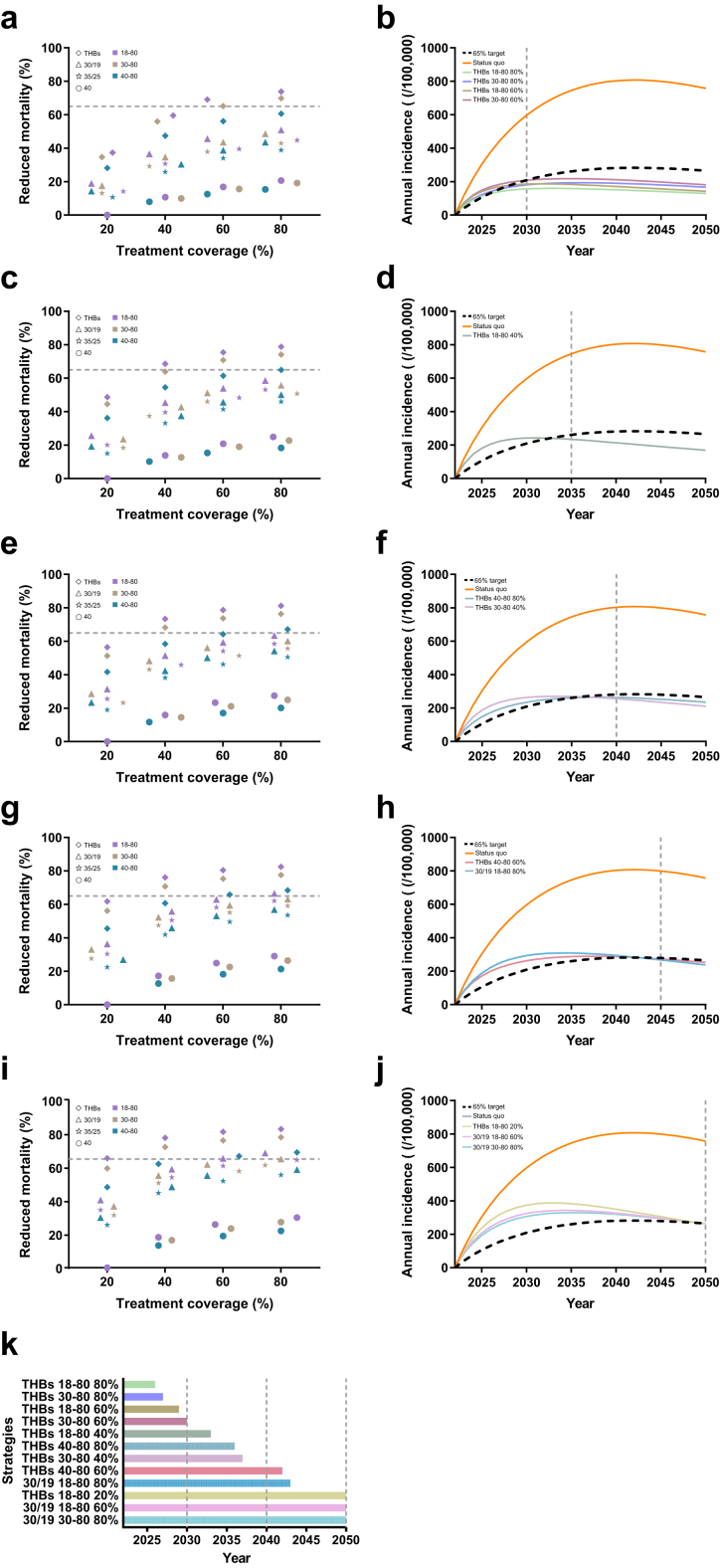
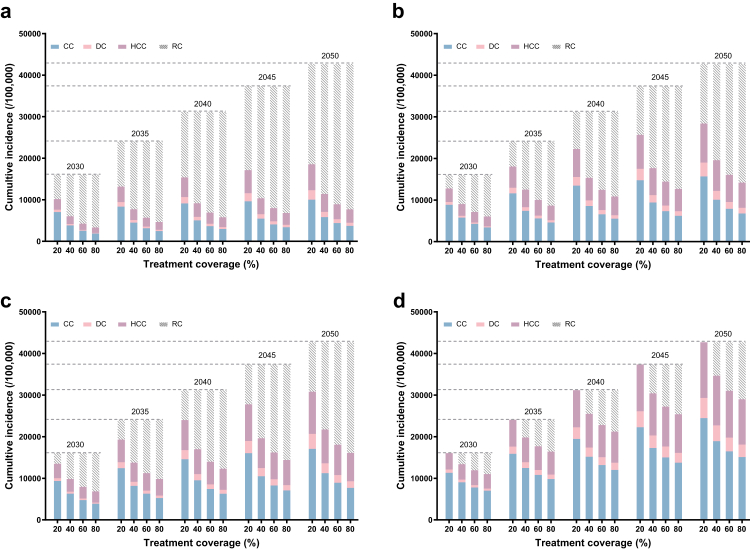
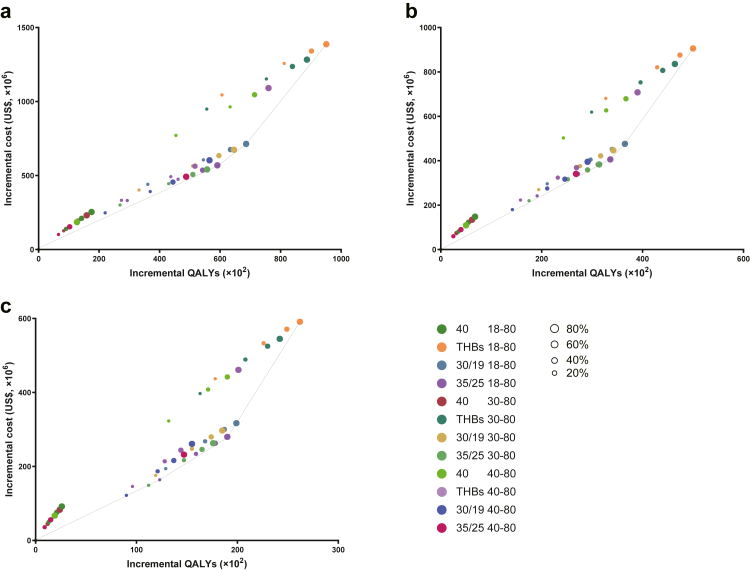
Findings: Besides the status quo, we finally simulated 135 treatment-expanding scenarios based on the cross combination of different thresholds of ALT, treatment coverages, population's age groups and implementation time. For the status quo, a cumulative incidence of 16,038-42,691 HBV-related complications and 3116-18,428 related deaths will happened between 2030 and 2050. When the treatment threshold is expanded to 'ALT > 35 in males & ALT > 25 in females' immediately without expanding treatment coverage, it will save 2554 HBV-related complications and 348 related deaths compared to the status quo among the whole cohort by 2030, and US$ 156 million more will be costed for gaining 2962 more QALYs. If we just expand the ALT threshold to ALT > 30 in males & ALT > 19 in females, 3247 HBV-related complications and 470 related deaths will be prevented by 2030 under the current treatment coverage of 20%, which will cost US$ 242 million, US$ 583 million or US$ 606 million more by the year of 2030, 2040 or 2050, respectively. Treatment expanded to HBsAg+ will save the largest number of HBV-related complications and death. This expanding strategy also results in large complications or death reduction when it is limited to patients older than 30 years or 40 years. Under this strategy, four scenarios (Treating HBsAg+ with coverage of 60% or 80% for patients older than 18 years or 30 years) showed the effectiveness in reaching the target before the year 2030. Among all the strategies, treatment expanded to HBsAg+ would cost the most while providing the highest total QALYs compared to other strategies with similar implementation scenarios. ALT thresholds of 30 U/L and 19 U/L for males and females, respectively, with 80% coverage for 18-80 years, can attain the goal by 2043.
Interpretation: Treating HBsAg+ individuals with 80% coverage for 18-80 years is optimal; earlier implementation of expanded antiviral treatment with a modified ALT threshold could decrease HBV-related complications and deaths to support the global target of 65% reduction in viral hepatitis B deaths.
Funding: This study was funded by Global Center for Infectious Disease and Policy Research (BMU2022XY030); Global Health and Infectious Diseases Group (BMU2022XY030); The Chinese Foundations for Hepatitis Control and Prevention (2021ZC032); National Science and Technology Project on Development Assistance for Technology, Developing China-ASEAN Public Health Research and Development Collaborating Center (KY202101004); in part by National Key R&D Program of China (2022YFC2505100).
Keywords: Alanine transaminase; Chronic HBV infection; Cost-effectiveness; Treatment.
© 2023 The Author(s).
Conflict of interest statement
FQC is a staff member of Chinese Foundation for hepatitis Control and prevention and has received research funding from Chinese Foundation for hepatitis Control and prevention. All other authors declare no competing interests.
Figures
References
-
- Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Accountability for the global health sector strategies 2016–2021: actions for impact. 2021. http://www.who.int/hepatitis/strategy2016-2021/ghss-hep/en/
-
- Authors/Task Force M, Guidelines ESCCfP, Societies ESCNC 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Atherosclerosis. 2019;290:140–205. - PubMed
-
- Easterbrook P., Luhmann N., Newman M., Walsh N., Lesi O., Doherty M. New WHO guidance for country validation of viral hepatitis B and C elimination. Lancet Gastroenterol Hepatol. 2021;6(10):778–780. - PubMed
LinkOut - more resources
Full Text Sources
