

Prehospital Antibiotics Improve Morbidity and Mortality of Emergency Medical Service Patients with Sepsis
- PMID: 37424716
- PMCID: PMC10324699
- DOI: 10.36518/2689-0216.1063
Prehospital Antibiotics Improve Morbidity and Mortality of Emergency Medical Service Patients with Sepsis
Abstract
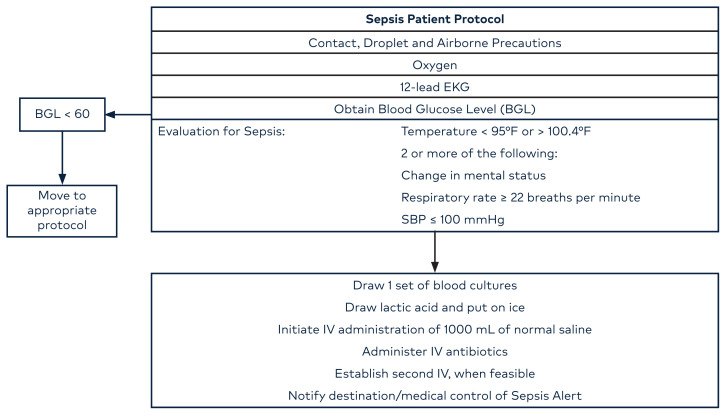
Background: Severe sepsis is a major cause of mortality in patients evaluated in the Emergency Department (ED). Early initiation of antibiotic therapy and IV fluids in the ED is associated with improved outcomes. We investigated whether early administration of antibiotics in the prehospital setting improves outcomes in these patients with sepsis.
Methods: This is a retrospective study comparing outcomes of patients meeting sepsis criteria in the field by EMS, who were treated with IV fluids and antibiotics. Their outcomes were compared with controls where fluids were administered prehospital and antibiotics were initiated in the ED. We compared morbidity and mortality between these groups.
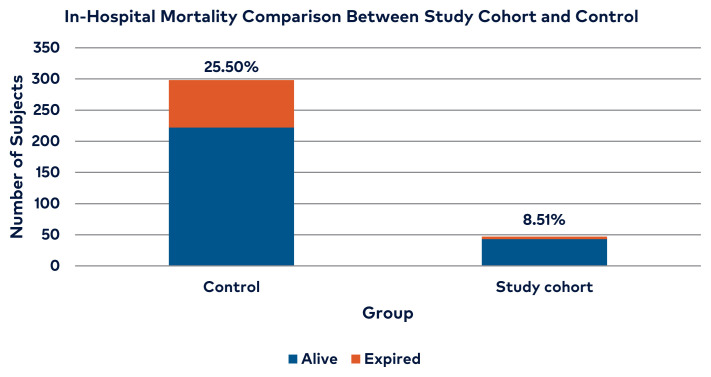
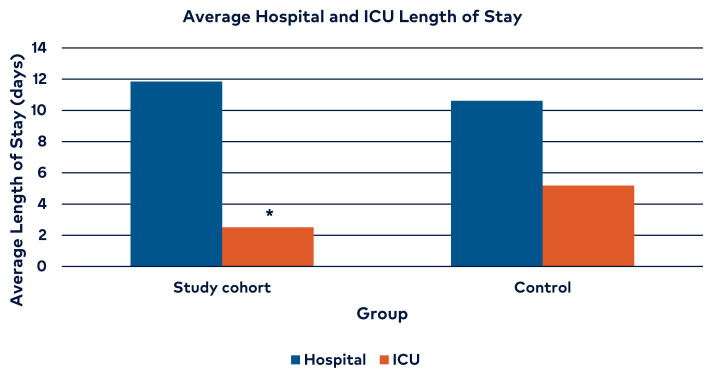
Results: Early antibiotics and fluids were demonstrated to show significant improvement in outcomes in the patients meeting sepsis criteria treated in the pre-hospital setting. The average age for sepsis patients receiving antibiotics in the prehospital setting was statistically higher than that for patients in the historical control group, 73.23 years and 67.67, respectively (p < 0.036), and there was no statistically significant difference of Charlson Comorbidity Index between the groups (p two-tail = 0.28). Average intensive care unit length of stay was 2.51 days in the in the prehospital group and 5.18 days in the historical controls, and the prehospital group received fewer blood products than the historical controls (p = 0.0003).
Conclusions: Early IV administration of antibiotics in the field significantly improves outcome in EMS patients who meet sepsis criteria based on a modified qSOFA score.
Keywords: Emergency Medical Services; antibiotic prophylaxis; antibiotics; emergency treatment; prehospital; retrospective studies; sepsis/diagnosis; sepsis/therapy; time factors.
© 2020 HCA Physician Services, Inc. d/b/a Emerald Medical Education.
Conflict of interest statement
Conflicts of Interest The authors declare they have no conflicts of interest.
Figures
Similar articles
-
Low sensitivity of qSOFA, SIRS criteria and sepsis definition to identify infected patients at risk of complication in the prehospital setting and at the emergency department triage.Scand J Trauma Resusc Emerg Med. 2017 Nov 3;25(1):108. doi: 10.1186/s13049-017-0449-y. Scand J Trauma Resusc Emerg Med. 2017. PMID: 29100549 Free PMC article.
-
Study protocol for a Multi-centre, Investigator-initiated, Randomized Controlled Trial to Compare the Effects of Prehospital Antibiotic Treatment for Sepsis Patients with Usual Care after Training Emergency Medical Services (EMS) Personnel in Early Recognition (- The Prehospital ANTibiotics Against Sepsis (PHANTASi) trial.Acute Med. 2016;15(4):176-184. Acute Med. 2016. PMID: 28112286 Clinical Trial.
-
qSOFA Has Poor Sensitivity for Prehospital Identification of Severe Sepsis and Septic Shock.Prehosp Emerg Care. 2017 Jul-Aug;21(4):489-497. doi: 10.1080/10903127.2016.1274348. Epub 2017 Jan 25. Prehosp Emerg Care. 2017. PMID: 28121217
-
Suspicion and treatment of severe sepsis. An overview of the prehospital chain of care.Scand J Trauma Resusc Emerg Med. 2012 Jun 27;20:42. doi: 10.1186/1757-7241-20-42. Scand J Trauma Resusc Emerg Med. 2012. PMID: 22738027 Free PMC article. Review.
-
Can Prehospital Data Improve Early Identification of Sepsis in Emergency Department? An Integrative Review of Machine Learning Approaches.Appl Clin Inform. 2022 Jan;13(1):189-202. doi: 10.1055/s-0042-1742369. Epub 2022 Feb 2. Appl Clin Inform. 2022. PMID: 35108741 Free PMC article. Review.
Cited by
-
Prehospital administration of broad-spectrum antibiotics for sepsis patients: A systematic review and meta-analysis.Health Sci Rep. 2022 Apr 1;5(3):e582. doi: 10.1002/hsr2.582. eCollection 2022 Apr. Health Sci Rep. 2022. PMID: 35387313 Free PMC article.
-
Sepsis management in pre-hospital care - the earlier, the better?BMC Emerg Med. 2024 Nov 19;24(1):220. doi: 10.1186/s12873-024-01137-0. BMC Emerg Med. 2024. PMID: 39563231 Free PMC article.
-
Impact of Prehospital Antibiotics on in-Hospital Mortality in Emergency Medical Service Patients with Sepsis.Open Access Emerg Med. 2023 May 26;15:199-206. doi: 10.2147/OAEM.S413791. eCollection 2023. Open Access Emerg Med. 2023. PMID: 37260737 Free PMC article.
References
-
- Hilditch M. Can pre-hospital recognition and intervention improve outcome for patients with severe sepsis? Journal of Paramedic Practice. 2015;7(4):168–75. doi: 10.12968/jpar.2015.7.4.168. - DOI
LinkOut - more resources
Full Text Sources